
Active Finding Development Model of Sampling Quality Improvement Model Using Nasopharyngeal Swab and Throat Swab for Active Finding of Persons Exposed to COVID-19 by Medical technologists and Multidisciplinary Care Teams at Taphraya District, Sa Kaeo Province
Keywords:
Quality improvement, SARS-CoV-2 (COVID-19) sampling collection, Proactive screening model for people exposed to COVID-19Abstract
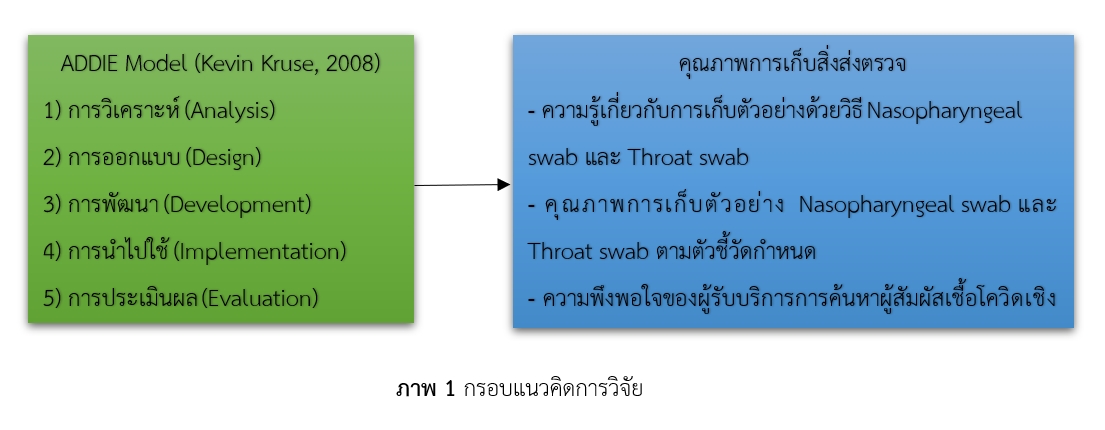
The COVID outbreak has necessitated the mobilization of manpower from diverse fields to gather samples from various demographic groups, resulting in variations of sample quality. The aims of this research were to assess the quality enhancement of sample collection for SARS-CoV-2 (COVID-19) testing and to examine the strategy for proactive identifying individuals exposed to COVID-19 infection with the involvement of medical technicians and multidisciplinary care teams at Ta Phraya district, Sa Kaeo province. Research and development (R&D) in conjunction with systematic instruction based on the "ADDIE Model" was employed to conduct this study with samples of 30 multidisciplinary personnel. The samples involved in a five-step research process: 1) context and problem analysis; 2) designing and development of quality process; 3) model development; 4) model application; and 5) model evaluation. Data collection was conducted through the administration of questionnaires and performance evaluation forms. Data were analyzed using one group pre-posttest design.
The results revealed that after applying the developed model, the multidisciplinary care teams exhibited higher the average scores in their knowledge and practical skills related to specimen collection using the Nasopharyngeal swab and Throat swab methods about 3.27 points (S.D.=3.03) with statistically significant difference (P<0.001). The criteria for specimen rejection rate, set as at a maximum of 1%, was successfully met at 0%. Moreover, the accuracy in submitting samples for SAR-CoV-2 testing via the Real time RT-PCR method was met at 100%, aligning with the setting goal. This resulted in 92% satisfaction rate among those receiving further testing for SAR-CoV-2 infection using the Real time RT-PCR method, exceeding the goal of 85%. A model for proactive identification of COVID-19 exposure of the individuals had been refined into a 4-step process, leading to a substantial reduction of 1.30 hours in waiting times. This improvement not only enhances the quality of SARS-CoV-2 (COVID-19) sample collection, but also establishes a structured approach for identifying individuals exposed to COVID-19 infection. The multidisciplinary care teams can apply this model as a potential prototype for other projects.
References
กรมควบคุมโรค. (2564). สถานการณ์ผู้ติดเชื้อ COVID-19. [ออนไลน์]. 2564; [สืบค้น 31 ส.ค. 2564]; [1 หน้า]. เข้าถึงได้ที่: URL:http://ddc.moph.go.th/covid19-dashboard/.
กลุ่มงานพัฒนาคุณภาพและวิชาการ โรงพยาบาลตาพระยา. (2564). สรุปผลงานประจำปี 2564 การประชุมคณะกรรมการบริหาร และทีมนำทางคุณภาพ. สระแก้ว : โรงพยาบาลตาพระยา จังหวัดสระแก้ว.
กุศลาสัย สุราอามาตย์ สงครามชัย ลีทองดี และเสฐียรพงษ์ ศิวินา (2562), รูปแบบการพัฒนาคุณภาพห้องปฏิบัติการด้านการแพทย์และสาธารณสุข ตามเกณฑ์มาตรฐานโรงพยาบาลส่งเสริมสุขภาพตำบลติดดาว ในเครือข่ายบริการปฐมภูมิ อำเภอจตุรพักตรพิมาน จังหวัดร้อยเอ็ด. วารสารโรงพยาบาลมหาสารคาม ปีที่ 16 ฉบับที่ 1 (มกราคม - เมษายน) พ.ศ. 2562.
คณะแพทยศาสตร์โรงพยาบาลรามาธิบดี มหาวิทยาลัยมหิดล.ประสบการณ์เตรียมห้องปฏิบัติการทางการแพทย์ พร้อมรับโรค COVID-19 [ออนไลน์]. 2564; [สืบค้น 20 ส.ค. 2564]; [1 หน้า]. เข้าถึงได้ที่: URL:http://med.mahidol.ac.th/atrama/issue037/open-lab
ชลอวัฒน์ อินปา และ พิศิษฐ์ ศรีประเสริฐ. (2564). ความชุกและปัจจัยที่สัมพันธ์กับภาวะเครียดและซึมเศร้าในบุคลากรทางการแพทย์โรงพยาบาลสมเด็จพระเจ้าตากสินมหาราชในช่วงการแพร่ระบาดโรค COVID-19. เชียงรายเวชสาร, 13(2), 153-165.
นภสร ดวงสมสา และคณะ. (2556). ผลของการพัฒนาคุณภาพโดยทีมพยาบาลต่ออัตราการปนเปื้อนเชื้อจุลชีพในเลือดที่ส่งตรวจเพาะเชื้อ. พยาบาลสาร ปีที่ 40 ฉบับที่ 4 ตุลาคม-ธันวาคม พ.ศ. 2556 ; 12-21.
บี บี ซี นิวส์ ไทย.โควิด-19: ลำดับเหตุการณ์ แผนที่ อินโฟกราฟิก ยอดติดเชื้อ-เสียชีวิตในไทยและทั่วโลก [ออนไลน์]. 2564; [สืบค้น 31 ส.ค. 2564]; [1 หน้า]. เข้าถึงได้ที่: URL:https://www.bbc.-com/thai/thailand-52090088
ปรียะดา ภัทรสัจจธรรม. (2559). การออกแบบการเรียนการสอนเชิงระบบโดยใช้แบบจำลอง ADDIE : การพัฒนาการคิดแบบเมตาคอกนิชัน (Metacognition) ของนักศึกษาพยาบาล. วารสารศึกษาศาสตร มหาวิทยาลัยศิลปากร ปที่ 13 ฉบับที่ 2 (พฤศจิกายน 2558-มีนาคม 2559) หน้า 6-17
มหาวิทยาลัยมหิดล. (2563). ความรู้พื้นฐาน COVID - 19 การติดเชื้ออการป่วย การดูแลรักษา การป้องกันการแพร่เชื้อและการติดเชื้อ. กรุงเทพมหานคร: มหาวิทยาลัยมหิดล.
Kruse, K. (2008). Introduction to Instructional Design and the ADDIE Model. [Online]
Accessed 30 December . Available from http://www.elearningguru.com/ articles/art2.
Sripraphan, M. Basic Knowledge of Antigen Test Kit for Screening for COVID-19. Retrieved
April 8, 2021 from http:// pharmacy.mahidol.ac.th/knowledge/files/0570.pdf
World Health Organization. Coronavirus disease (COVID-19) technical guidance: laboratory testing for 2019-nCoV in humans. [online]. 2020; [cited 2020 Jun 20]; [5 screens]. Available from: URL: https://www.who.int/emergencies/diseases/novel-%ADcoronavirus-%AD2019/technical-%ADguidance/laboratory-%ADguidance.
Downloads
Published
Issue
Section
License
Copyright (c) 2024 Journal of Council of Community Public Health

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
- บทความหรือข้อคิดเห็นใด ๆ ที่ปรากฏในวารสารสภาการสาธารณสุขชุมชน ที่เป็นวรรณกรรมของผู้เขียน บรรณาธิการ ไม่จำเป็นต้องเห็นด้วย
- บทความที่ได้รับการตีพิมพ์ถือเป็นลิขสิทธิ์ของ วารสารสภาการสาธารณสุขชุมชน

