
Clinical Prediction Model for Hypokalemia in Hospitalized Patients with Acute Decompensated Heart Failure Treated with Intravenous Furosemide
Article Sidebar
Main Article Content
Abstract
Background: Hospitalized patients with acute heart failure often receive furosemide, which may lead to hypokalemia. Factors such as diuretic dose and concomitant use of multiple diuretics are associated with this risk. This study aimed to develop a clinical prediction model for hypokalemia to help prevent its occurrence and related complications.
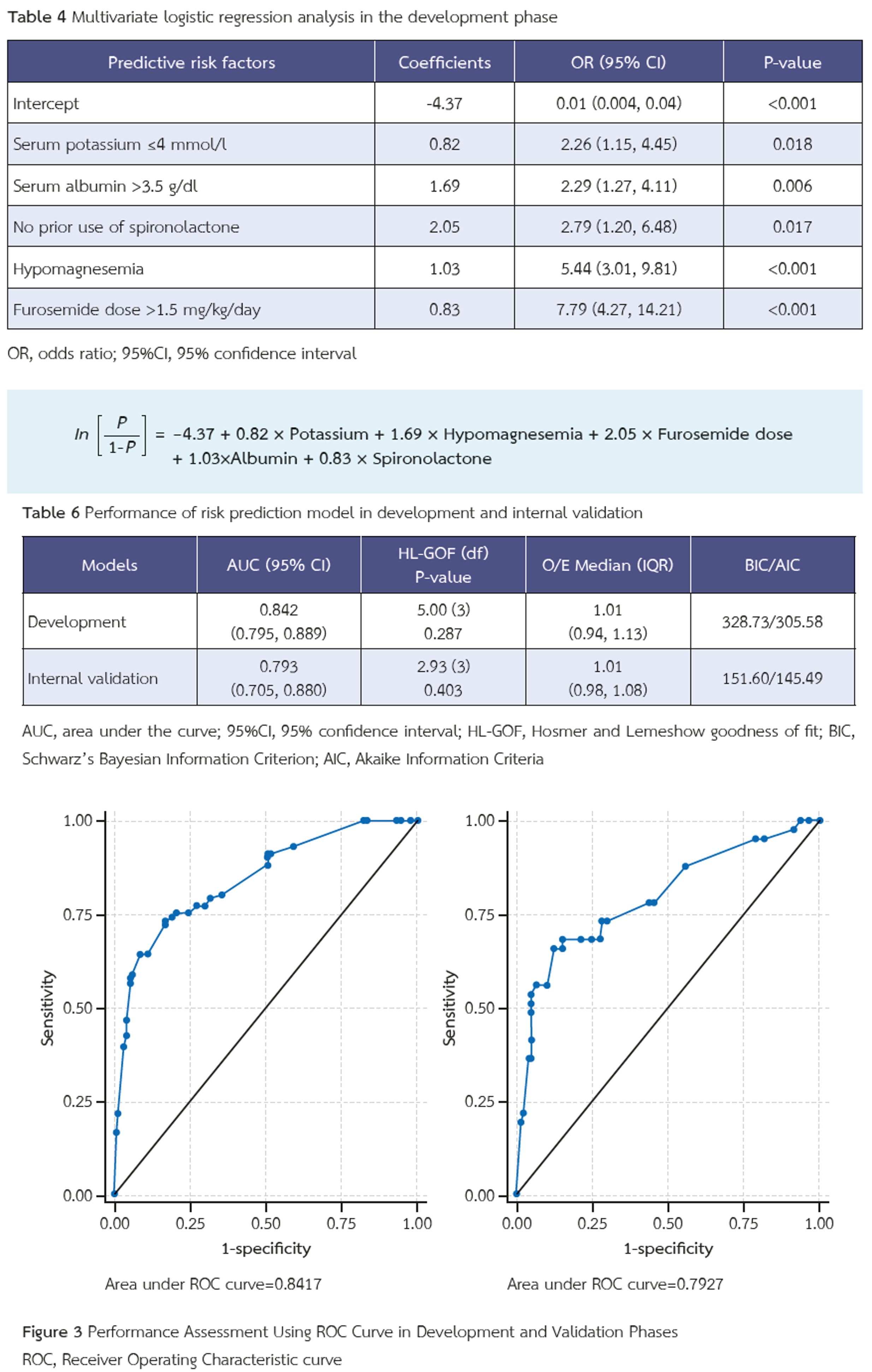
Methods: This is a retrospective clinical study of hospitalized patients with acute decompensated heart failure (ADHF). Using multivariable logistic regression, we derived a prediction score by assigning weights to the predictor coefficients. The score was then internally validated to assess its reliability.
Results: Among 510 hospitalized patients with ADHF receiving furosemide, 143 (28%) developed hypokalemia. Furosemide doses >1.5 mg/kg/day were strongly associated with hypokalemia (adjusted OR 4.81, 95% CI 2.56–9.04, p <0.001). Five predictors were identified: baseline serum potassium <4 mmol/L, serum albumin >3.5 g/dL, low serum magnesium, furosemide dose >1.5 mg/kg, and no prior spironolactone use. Higher scores were associated with an increased risk of hypokalemia.
Conclusions: The clinical prediction model provides a practical tool for estimating the risk of hypokalemia. ADHF
patients identified as high risk may benefit from preventive strategies and closer monitoring of potassium levels.
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This article is published under CC BY-NC-ND 4.0 license, which allows for non-commercial reuse of the published paper as long as the published paper is fully attributed. Anyone can share (copy and redistribute) the material in any medium or format without having to ask permission from the author or the Nephrology Society of Thailand.
References
Joseph SM, Cedars AM, Ewald GA, Geltman EM, Mann DL. Acute decompensated heart failure: contemporary medical management. Tex Heart Inst J. 2009;36(6):510-20.
Thu Kyaw M, Maung ZM. Hypokalemia-Induced Arrhythmia: A Case Series and Literature Review. Cureus. 2022;14(3):e22940. doi: 10.7759/cureus.22940
Krogager ML, Søgaard P, Torp-Pedersen C, Bøggild H, Lee CJ, Bonde A, et al. Impact of plasma potassium normalization on short-term mortality in patients with hypertension and hypokalemia or low normal potassium. BMC Cardiovasc Disord. 2020;20(1):386. doi: 10.1186/s12872-020-01654-3
Kim MJ, Valerio C, Knobloch GK. Potassium Disorders: Hypokalemia and Hyperkalemia. Am Fam Physician. 2023;107(1):59-70.
Brueske B, Sidhu MS, Schulman-Marcus J, Kashani KB, Barsness GW, Jentzer JC. Hyperkalemia Is Associated With Increased Mortality Among Unselected Cardiac Intensive Care Unit Patients. J Am Heart Assoc. 2019;8(7):e011814. doi: 10.1161/jaha.118.011814
Lin Z, Wong LYF, Cheung BMY. Diuretic-induced hypokalaemia: an updated review. Postgrad Med J. 2022;98(1160):477-82. doi: 10.1136/postgradmedj-2020-139701
Aimbudlop K, Saengpanit D. Factors Associated with Hypokalemia after Furosemide Treatment in Hospitalized Patients with Acute Decompensated Heart Failure. J Nephrol Soc Thail. 2024;30(1):57-68.
Metcalfe C. Biostatistics: A Foundation for Analysis in the Health Sciences. 7th edn. Wayne W. Daniel, Wiley, 1999. No. of. pages: xiv+755+appendices. ISBN 0-471-16386-4. Statistics in Medicine - STAT MED. 2001;20:324-6. doi: 10.1002/1097-0258(20010130)20:2<324::aid-sim635>3.0.co;2-o
Kapelios CJ, Kaldara E, Ntalianis A, Sousonis V, Repasos E, Sfakianaki T, et al. High furosemide dose has detrimental effects on survival of patients with stable heart failure. Hellenic J Cardiol. 2015;56(2):154-9.
Weiner ID, Wingo CS. Hypokalemia--consequences, causes, and correction. J Am Soc Nephrol. 1997;8(7):1179-88. doi: 10.1681/asn.v871179
Huang CL, Kuo E. Mechanism of hypokalemia in magnesium deficiency. J Am Soc Nephrol. 2007;18(10):2649-52. doi: 10.1681/asn.2007070792
Brater DC. Diuretic therapy. N Engl J Med. 1998;339(6):387-95. doi: 10.1056/nejm199808063390607
Vardeny O, Claggett B, Anand I, Rossignol P, Desai AS, Zannad F, et al. Incidence, predictors, and outcomes related to hypo- and hyperkalemia in patients with severe heart failure treated with a mineralocorticoid receptor antagonist. Circ Heart Fail. 2014;7(4):573-9. doi: 10.1161/circheartfailure.114.001104
Epstein M, Calhoun DA. Aldosterone blockers (mineralocorticoid receptor antagonism) and potassium-sparing diuretics. J Clin Hypertens (Greenwich). 2011;13(9):644-8. doi: 10.1111/j.1751-7176.2011.00511.x
Kieneker LM, Eisenga MF, Joosten MM, de Boer RA, Gansevoort RT, Kootstra-Ros JE, et al. Plasma potassium, diuretic use and risk of developing chronic kidney disease in a predominantly White population. PLoS One. 2017;12(3):e0174686. doi: 10.1371/journal.pone.0174686
Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr., Colvin MM, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017;136(6):e137-e61. doi: 10.1161/cir.0000000000000509
