
Factors Associated with Hypokalemia after Furosemide Treatment in Hospitalized Patients with Acute Decompensated Heart Failure
Article Sidebar
Main Article Content
Abstract
Background: Hypokalemia, defined as serum potassium <3.5 mmol/L, is commonly associated with the use of loop diuretics. Hypokalemia after furosemide treatment may lead to adverse outcomes in hospitalized patients with acute decompensated heart failure (ADHF). Risk factors associated with hypokalemia in this patient population are not well characterized. This retrospective case-control study aimed to identify risk factors and outcomes associated with hypokalemia after furosemide treatment in hospitalized patients with ADHF.
Methods: The data were retrieved from the medical records using ICD-10 coding. Factors associated with hypokalemia were analyzed using univariate and multivariate logistic regression analyses. Clinical outcomes associated with the hypokalemia were also examined.
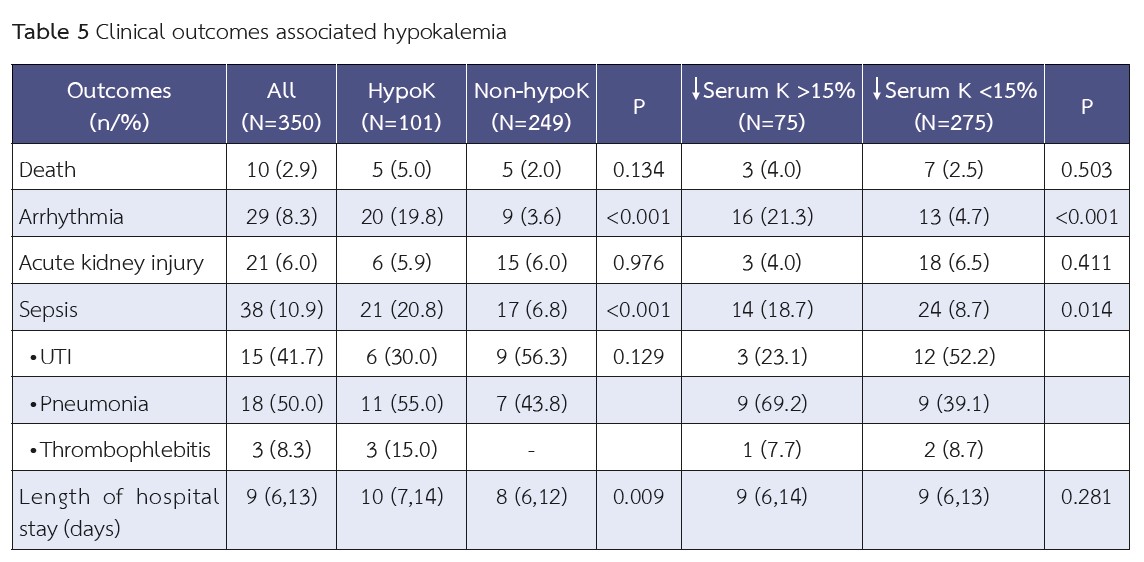
Results: A total of 350 patients met the eligibility criteria, of whom 101 patients developed hypokalemia after receiving furosemide, while 249 patients did not. Furosemide dose >1.5 mg/kg, urine volume after furosemide treatment >2 ml/kg/hour, higher baseline serum albumin and body mass index, the presence of baseline hypomagnesemia and lower baseline serum potassium were independently associated with hypokalemia after furosemide treatment. Prior use of spironolactone was associated with a decreased risk of hypokalemia. Patients in the hypokalemia group had significantly higher incidence of cardiac arrhythmia and sepsis compared with the non-hypokalemia group.
Conclusion: Close monitoring of serum potassium among high risk patients may help reduce the incidence of hypokalemia and adverse clinical outcomes in hospitalized patients with ADHF who received furosemide.
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This article is published under CC BY-NC-ND 4.0 license, which allows for non-commercial reuse of the published paper as long as the published paper is fully attributed. Anyone can share (copy and redistribute) the material in any medium or format without having to ask permission from the author or the Nephrology Society of Thailand.
References
Redfield MM. Heart failure with preserved ejection fraction. N Engl J Med. 2016:10;375(19):1868-77.
Jessup M, Brozena S. Heart failure. N Engl J Med. 2003;348(20):2007-18.
Wargo KA, Banta WM. A comprehensive review of the loop diuretics: should furosemide be first line?. Ann Pharmacother. 2009;43(11):1836-47.
Wu MY, Chang NC, Su CL, Hsu YH, Chen TW, Lin YF, et al. Loop diuretic strategies in patients with acute decompensated heart failure: a meta-analysis of randomized controlled trials. J Crit Care. 2014;29(1):2-9
Hussain M, Walton K, Davidson C, Morgan DB. A study of two diuretic/potassium combinations in heart failure. Postgrad Med J. 1985;61(711):29-33.
Cote JM, Bouchard J, Murray PT, Beaubien-Souligny W. Diuretic strategies in patients with resistance to loop-diuretics in the intensive care unit: A retrospective study from the MIMIC-III database. J Crit Care. 2021;65:282-91.
Tamargo J, Segura J, Ruilope LM. Diuretics in the treatment of hypertension. Part 2: loop diuretics and potassium-sparing agents. Expert Opin Pharmacother. 2014;15(5):605-21.
Collins AJ, Pitt B, Reaven N, Funk S, McGaughey K, Wilson D, et al. Association of serum potassium with all-cause mortality in patients with and without heart failure, chronic kidney disease, and/or diabetes. Am J Nephrol. 2017;46(3):213-21.
Bowling CB, Pitt B, Ahmed MI, Aban IB, Sanders PW, Mujib M, et al. Hypokalemia and outcomes in patients with chronic heart failure and chronic kidney disease: findings from propensity-matched studies. Circ Heart Fail. 2010;3(2):253-60.
Ikram HW, Chan W, Espiner EA, Nicholls MG. Haemodynamic and hormone responses to acute and chronic frusemide therapy in congestive heart failure. Clin Sci (Lond). 1980;59(6):443-9.
Cohn JN, Kowey PR, Whelton PK, Prisant LM. New guidelines for potassium replacement in clinical practice: a contemporary review by the National Council on Potassium in Clinical Practice. Arch Intern Med. 2000;160(16):2429-36.
Leonard CE, Razzaghi H, Freeman CP, Roy JA, Newcomb CW, Hennessy S. Empiric potassium supplementation and increased survival in users of loop diuretics. PloS one. 2014;9(7):e102279.
Kaplan NM, Carnegie A, Raskin P, Heller JA, Simmons M. Potassium supplementation in hypertensive patients with diuretic-induced hypokalemia. N Engl J Med. 1985;312(12):746-9.
Kellum JA, Lameire N, Aspelin P, Barsoum RS, Burdmann EA, Goldstein SL, et al. Kidney disease: improving global outcomes (KDIGO) acute kidney injury work group. Kidney Int Suppl. 2012;2(1):1-38.
Peduzzi P, Concato J, Feinstein AR, Holford TR. Importance of events per independent variable in proportional hazards regression analysis II. Accuracy and precision of regression estimates. J Clin Epidemiol. 1995;48(12):1503-10.
Reyes AJ. Effects of diuretics on outputs and flows of urine and urinary solutes in healthy subjects. Drugs. 1991;41 Suppl 3:35-59.
McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599-726.
Pitt B, Zannad F, Remme WJ, Cody R, Castaigne A, Perez A, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. N Engl J Med. 1999;341(10):709-17.
Zannad F, McMurray JJ, Krum H, van Veldhuisen DJ, Swedberg K, Shi H, et al. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med. 2011;364(1):11-21.
Sica DA. Pharmacokinetics and pharmacodynamics of mineralocorticoid blocking agents and their effects on potassium omeostasis. Heart Fail Rev. 2005;10:23-9.
Huang CL, Kuo E. Mechanism of hypokalemia in magnesium deficiency. J Am Soc Nephrol. 2007;18(10):2649-52.
Whang R, Ryder KW. Frequency of hypomagnesemia and hypermagnesemia: requested vs routine. JAMA. 1990;263(22):3063-4.
Mariosa LS, Ribeiro-Filho FF, Batista MC, Hirota AH, Borges RL, Ribeiro AB, et al. Abdominal obesity is associated with potassium depletion and changes in glucose homeostasis during diuretic therapy. J Clin Hypertens (Greenwich). 2008;10(6):443-9.
Duffy M, Jain S, Harrell N, Kothari N, Reddi AS. Albumin and furosemide combination for management of edema in nephrotic syndrome: a review of clinical studies. Cells. 2015;4(4):622-30.
Phakdeekitcharoen B, Boonyawat K. The added-up albumin enhances the diuretic effect of furosemide in patients with hypoalbuminemic chronic kidney disease: a randomized controlled study. BMC Nephrol. 2012;13:92.
Lowe J, Gray J, Henry DA, Lawson DH. Adverse reactions to frusemide in hospital inpatients. Br Med J. 1979;2(6186):360-2.
Kieneker LM, Eisenga MF, Joosten MM, de Boer RA, Gansevoort RT, Kootstra-Ros JE, et al. Plasma potassium, diuretic use and risk of developing chronic kidney disease in a predominantly White population. PloS one. 2017;12(3):e0174686.
Salah K, Pinto YM, Eurlings LW, Metra M, Stienen S, Lombardi C, et al. Serum potassium decline during hospitalization for acute decompensated heart failure is a predictor of 6-month mortality, independent of N-terminal pro–B-type natriuretic peptide levels: An individual patient data analysis. Am Heart J. 2015;170(3):531-42.
