
Sepsis-associated Acute Kidney Injury Subphenotypes in Critically Ill Patients by Staging Trajectories
Article Sidebar
Main Article Content
Abstract
Background: Sepsis is the leading cause of acute kidney injury (AKI) in critically ill patients. The current Kidney Disease: Improving Global Outcomes (KDIGO) criteria rely on maximal serum creatinine levels, which do not account for longitudinal changes. This study aimed to examine AKI staging trajectories and hypothesized that subphenotypes based on these trajectories are associated with different outcomes.
Methods: Two independent databases of patients in the intensive care unit (ICU) with AKI in Southeast Asia were analyzed. The SEA-AKI cohort served as the development cohort, while the KCMH cohort was used for validation. Group-based trajectory modelling identified subphenotypes of AKI staging in septic patients during the first seven days after ICU admission. Baseline characteristics, AKI staging, duration, recovery, and the occurrence and staging of acute kidney disease were compared between clusters. Associations between clusters and 28-day mortality, ICU and hospital mortality, and major adverse kidney events at day 28 (MAKE28) were evaluated.
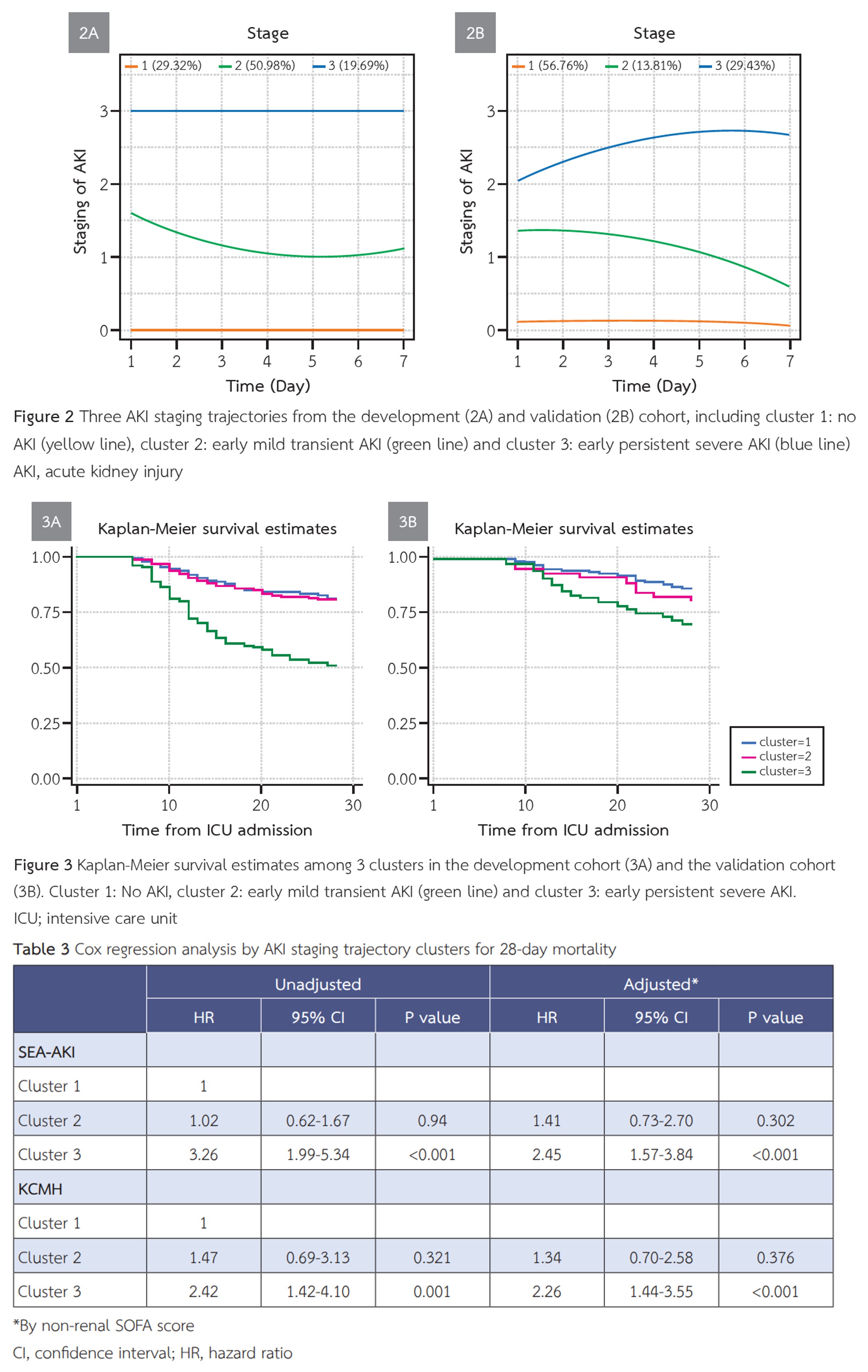
Results: A total of 457 patients were included in the development cohort and 333 in the validation cohort. AKI occurred in 70.7% of the development cohort and 63.4% of the validation cohort. Three distinct clusters of AKI staging trajectories were identified in the development cohort: Cluster 1 (No AKI, 29.3%), Cluster 2 (early mild transient AKI, 50.9%), and Cluster 3 (early severe persistent AKI, 19.7%). Compared with the other clusters, an independent association was found between Cluster 3 and increased 28-day mortality. These findings were confirmed in the validation cohort.
Conclusions: AKI staging trajectories identified distinct subphenotypes associated with different outcomes. Further studies are needed to explore subphenotype-based interventions.
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This article is published under CC BY-NC-ND 4.0 license, which allows for non-commercial reuse of the published paper as long as the published paper is fully attributed. Anyone can share (copy and redistribute) the material in any medium or format without having to ask permission from the author or the Nephrology Society of Thailand.
References
Hoste EA, Bagshaw SM, Bellomo R, Cely CM, Colman R, Cruz DN, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 2015;41(8):1411-23.
Jeong R, Haines R, Ostermann M. Outcomes after acute kidney injury and critical illness. Curr Opin Crit Care. 2024;30(5):502-9.
Mehta RL, Burdmann EA, Cerdá J, Feehally J, Finkelstein F, García-García G, et al. Recognition and management of acute kidney injury in the International Society of Nephrology 0by25 Global Snapshot: a multinational cross-sectional study. Lancet. 2016;387(10032):2017-25.
Zarbock A, Nadim MK, Pickkers P, Gomez H, Bell S, Joannidis M, et al. Sepsis-associated acute kidney injury: consensus report of the 28th Acute Disease Quality Initiative workgroup. Nat Rev Nephrol. 2023;19(6):401-17.
Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012;120(4):c179-84.
Kellum JA, Sileanu FE, Bihorac A, Hoste EA, Chawla LS. Recovery after Acute Kidney Injury. Am J Respir Crit Care Med. 2017;195(6):784-91.
Perinel S, Vincent F, Lautrette A, Dellamonica J, Mariat C, Zeni F, et al. Transient and Persistent Acute Kidney Injury and the Risk of Hospital Mortality in Critically Ill Patients: Results of a Multicenter Cohort Study. Crit Care Med. 2015;43(8):e269-75.
Takkavatakarn K, Oh W, Chan L, Hofer I, Shawwa K, Kraft M, et al. Machine learning derived serum creatinine trajectories in acute kidney injury in critically ill patients with sepsis. Crit Care. 2024;28(1):156.
Andrew BY, Pieper CF, Cherry AD, Pendergast JF, Privratsky JR, Mathew JP, et al. Identification of Trajectory-Based Acute Kidney Injury Phenotypes Among Cardiac Surgery Patients. Ann Thorac Surg. 2022;114(6):2235-43.
Horie R, Hayase N, Asada T, Yamamoto M, Matsubara T, Doi K. Trajectory pattern of serially measured acute kidney injury biomarkers in critically ill patients: a prospective observational study. Ann Intensive Care. 2024;14(1):84.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495-9.
Srisawat N, Kulvichit W, Mahamitra N, Hurst C, Praditpornsilpa K, Lumlertgul N, et al. The epidemiology and characteristics of acute kidney injury in the Southeast Asia intensive care unit: a prospective multicentre study. Nephrol Dial Transplant. 2020;35(10):1729-38.
Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801-10.
Sterne JA, White IR, Carlin JB, Spratt M, Royston P, Kenward MG, et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:b2393.
Závada J, Hoste E, Cartin-Ceba R, Calzavacca P, Gajic O, Clermont G, et al. A comparison of three methods to estimate baseline creatinine for RIFLE classification. Nephrol Dial Transplant. 2010;25(12):3911-8.
Chawla LS, Bellomo R, Bihorac A, Goldstein SL, Siew ED, Bagshaw SM, et al. Acute kidney disease and renal recovery: consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nat Rev Nephrol. 2017;13(4):241-57.
Nagin DS. Group-based trajectory modeling: an overview. Ann Nutr Metab. 2014;65(2-3):205-10.
Bhatraju PK, Cohen M, Nagao RJ, Morrell ED, Kosamo S, Chai XY, et al. Genetic variation implicates plasma angiopoietin-2 in the development of acute kidney injury sub-phenotypes. BMC Nephrol. 2020;21(1):284.
Titeca-Beauport D, Diouf M, Daubin D, Vong LV, Belliard G, Bruel C, et al. The combination of kidney function variables with cell cycle arrest biomarkers identifies distinct subphenotypes of sepsis-associated acute kidney injury: a post-hoc analysis (the PHENAKI study). Ren Fail. 2024;46(1):2325640.
Vasquez-Rios G, Oh W, Lee S, Bhatraju P, Mansour SG, Moledina DG, et al. Joint Modeling of Clinical and Biomarker Data in Acute Kidney Injury Defines Unique Subphenotypes with Differing Outcomes. Clin J Am Soc Nephrol. 2023;18(6):716-26.
Wiersema R, Jukarainen S, Vaara ST, Poukkanen M, Lakkisto P, Wong H, et al. Two subphenotypes of septic acute kidney injury are associated with different 90-day mortality and renal recovery. Crit Care. 2020;24(1):150.
Bhatraju PK, Mukherjee P, Robinson-Cohen C, O’Keefe GE, Frank AJ, Christie JD, et al. Acute kidney injury subphenotypes based on creatinine trajectory identifies patients at increased risk of death. Crit Care. 2016;20(1):372.
Abdel-Nabey M, Ghrenassia E, Mariotte E, Valade S, Morel G, Lemiale V, et al. Acute Kidney Injury Recovery Patterns in Critically Ill Patients: Results of a Retrospective Cohort Study. Crit Care Med. 2021;49(7):e683-e92.
Chaudhary K, Vaid A, Duffy Á, Paranjpe I, Jaladanki S, Paranjpe M, et al. Utilization of Deep Learning for Subphenotype Identification in Sepsis-Associated Acute Kidney Injury. Clin J Am Soc Nephrol. 2020;15(11):1557-65.
Su CC, Chen JY, Chen SY, Shiao CC, Neyra JA, Matsuura R, et al. Outcomes associated with acute kidney disease: A systematic review and meta-analysis. EClinicalMedicine. 2023;55:101760.
Bhatraju PK, Prince DK, Mansour S, Ikizler TA, Siew ED, Chinchilli VM, et al. Integrated Analysis of Blood and Urine Biomarkers to Identify Acute Kidney Injury Subphenotypes and Associations With Long-term Outcomes. Am J Kidney Dis. 2023;82(3):311-21.e1.
Bhatraju PK, Zelnick LR, Herting J, Katz R, Mikacenic C, Kosamo S, et al. Identification of Acute Kidney Injury Subphenotypes with Differing Molecular Signatures and Responses to Vasopressin Therapy. Am J Respir Crit Care Med. 2019;199(7):863-72.
