
การศึกษาประสิทธิภาพของยาต้านการทำงาน Sodium-Glucose Co-transporter 2 ต่อการทำงานของไตในผู้ป่วยโรคไตเรื้อรังจากเบาหวาน
Article Sidebar
Main Article Content
บทคัดย่อ
บทนำ : โรคไตจากเบาหวานเป็นสาเหตุหลักของโรคไตเรื้อรังในประชากรทั่วโลก ยากลุ่ม sodium-Glucose Co-transporter 2 Inhibitors (SGLT2i) เป็นยาเบาหวานกลุ่มใหม่ที่นอกจากการจะลดระดับน้ำตาลในเลือดได้ ยังสามารถชะลอการเสื่อมของไตได้อีกด้วย อย่างไรก็ตามพบว่าประสิทธิภาพในการชะลอการเสื่อมของไตมีความแตกต่างกันในแต่ละภูมิภาค ในปัจจุบันยังไม่มีการศึกษาถึงประสิทธิภาพของยา SGLT2i ในประชากรไทยที่เป็นโรคไตจากเบาหวาน
วิธีการศึกษา : เป็นการศึกษาตามรุ่นย้อนหลังโดยมีกลุ่มเปรียบเทียบของผู้ป่วยที่มีโรคไตจากเบาหวานระหว่างวันที่ 1 มกราคม 2558 ถึง 31 ธันวาคม 2563 ผู้ป่วยที่มีโรคไตจากเบาหวานจะถูกแบ่งเป็น 2 กลุ่ม ได้แก่ กลุ่มที่ได้รับยา SGLT2i และ กลุ่มที่ไม่ได้รับยา ผู้ป่วยทั้งหมดจะได้รับการจับคู่ตาม อายุ, เพศ, การทำงานไต (estimate glomerular filtration rate, eGFR), ระดับอัลบูมินในปัสสาวะ และการได้รับยาในกลุ่ม renin angiotensin aldosterone inhibitors (RAASi) โดยมีผลลัพธ์หลักที่สนใจ คือ ความแตกต่างของ eGFR ที่ 96 สัปดาห์ระหว่างกลุ่มผู้ป่วยที่ได้รับ SGLT2i กับกลุ่มที่ไม่ได้รับยา และ ผลลัพธ์รอง คือ การเปลี่ยนแปลงของ eGFR และระดับอัลบูมินในปัสสาวะ รวมไปถึงอาการไม่พึงประสงค์
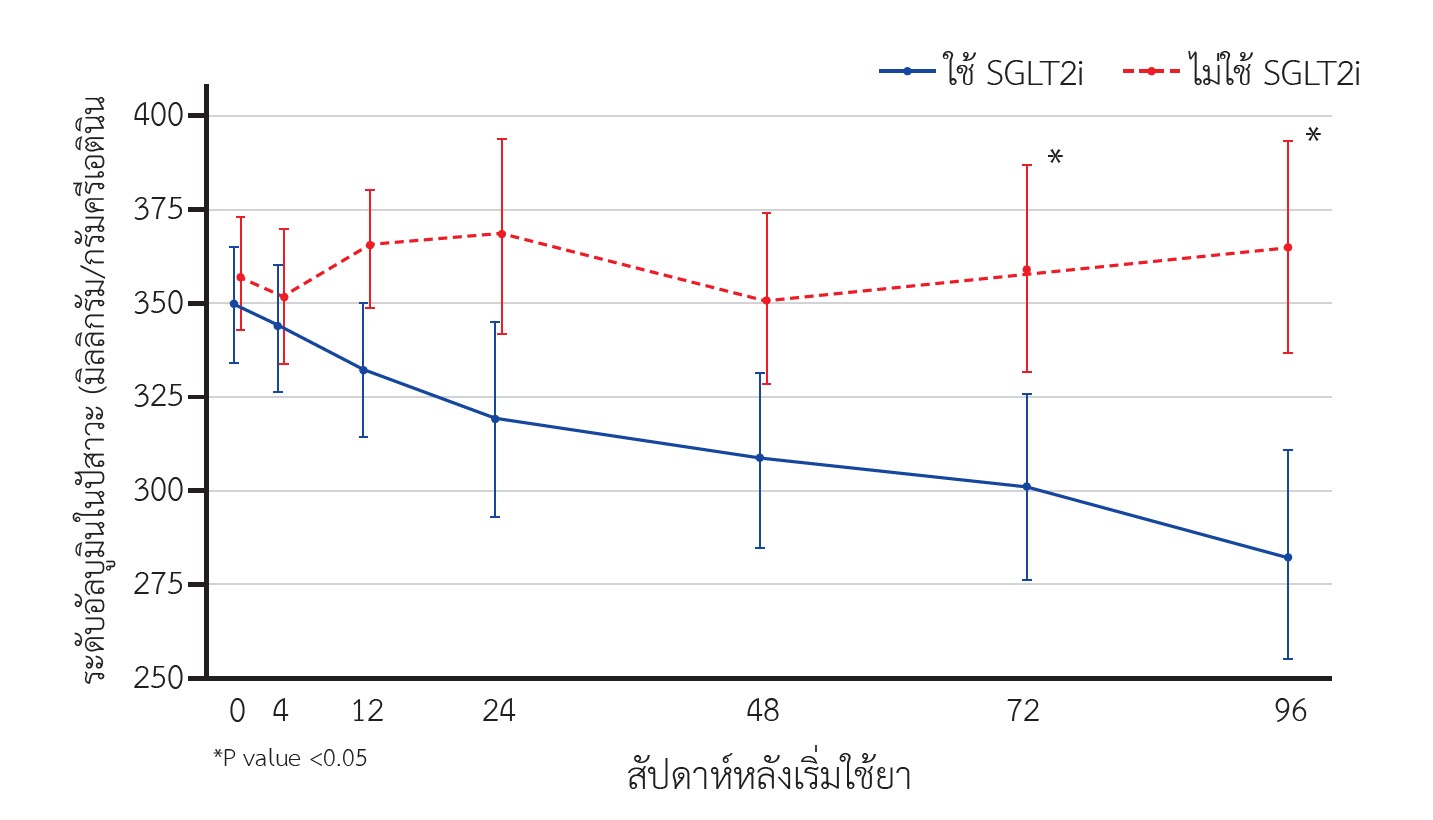
ผลการศึกษา : ผู้ป่วยในแต่ละกลุ่มมีจำนวน 180 คน ผู้ป่วยทั้ง 2 กลุ่มมีระดับ eGFR และอัลบูมินในปัสสาวะแรกเริ่มเท่าเทียมกัน จำนวนผู้ป่วยที่ใช้ RAASi ไม่แตกต่างกัน ผลการศึกษาหลักพบว่ากลุ่มผู้ป่วยที่ได้รับ SGLT2i มีระดับ eGFR ที่ 96 สัปดาห์สูงกว่ากลุ่มผู้ไม่ได้รับยาอย่างมีนัยสำคัญทางสถิติ (72.31 และ 65.37 มล./นาที/1.73 ตรม., P=0.031) และพบว่า กลุ่มผู้ป่วยที่ได้รับ SGLT2i มีการลดลงของ eGFR ที่ 96 สัปดาห์น้อยกว่ากลุ่มที่ไม่ได้รับยา (-4.76 vs -8.46 มล./นาที/1.73ตรม., p = 0.001) นอกจากนี้กลุ่มผู้ป่วยที่ได้รับ SGLT2i มีระดับอัลบูมินในปัสสาวะที่ 72 และ 96 สัปดาห์ ต่ำกว่ากลุ่มที่ไม่ได้รับยา การวิเคราะห์กลุ่มย่อยพบว่า กลุ่มผู้ป่วยที่ได้รับ SGLT2i ที่มีระดับ eGFR สูงกว่าที่ 96 สัปดาห์ เป็นกลุ่มผู้ป่วยที่มีค่า eGFR ตั้งต้น ≥90 มล./นาที/1.73 ตรม. เท่านั้น ผู้ป่วยที่ได้รับ SSGLT2i มีอุบัติการณ์การติดเชื้อทางเดินปัสสาวะสูงกว่า (P = 0.003) และไม่พบผลข้างเคียงรุนแรงอื่นในทั้ง 2 กลุ่ม
สรุป : การใช้ยา SGLT2i มีความสัมพันธ์กับการชะลอการเสื่อมของไตและการเพิ่มขึ้นปริมาณโปรตีนในปัสสาวะในผู้ป่วยโรคไตจากเบาหวาน การใช้ยา SGLT2i มีความสัมพันธ์กับอุบัติการณ์การติดเชื้อทางเดินปัสสาวะที่สูงขึ้น ในขณะที่ไม่พบผลข้างเคียงที่รุนแรงอื่น
Article Details

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
บทความนี้ตีพิมพ์ภายไต้การอนุญาต CC BY-NC-ND 4.0 ซึ่งอนุญาตให้สามารถใช้บทความนี้พื่อวัตถุประสงค์ใดๆ ก็ตามที่ไม่ใช่เชิงพาณิชย์ โดยต้องมีการอ้างถึงที่มาของบทความอย่างครบถ้วน ใครก็ตามสามารถคัดลอกและแจกจ่ายทุกส่วนของบทความนี้โดยไม่ต้องขออนุญาตจากผู้ประพันธ์หรือสมาคมโรคไตแห่งประเทศไทย
เอกสารอ้างอิง
Aekplakorn W, Chariyalertsak S, Kessomboon P, Sangthong R, Inthawong R, Putwatana P, et al. Prevalence and management of diabetes and metabolic risk factors in Thai adults: the Thai National Health Examination Survey IV, 2009: The Thai national health examination survey IV, 2009. Diabetes Care. 2011;34(9):1980–5.
Dall TM, Yang W, Gillespie K, Mocarski M, Byrne E, Cintina I, et al. The economic burden of elevated blood glucose levels in 2017: Diagnosed and undiagnosed diabetes, gestational diabetes mellitus, and prediabetes. Diabetes Care. 2019;42(9):1661–8.
Cao Z, Cooper ME. Pathogenesis of diabetic nephropathy: Pathogenesis of diabetic nephropathy. J Diabetes Investig. 2011;2(4):243–7.
Karalliedde J, Gnudi L. Endothelial factors and diabetic nephropathy. Diabetes Care. 2011;34:S291-6.
KDOQI. KDOQI clinical practice guidelines and clinical practice recommendations for diabetes and chronic kidney disease. Am J Kidney Dis. 2007;49(2 Suppl 2):S12-154.
Molitch ME, Adler AI, Flyvbjerg A, Nelson RG, So W-Y, Wanner C, et al. Diabetic kidney disease: a clinical update from Kidney Disease: Improving Global Outcomes. Kidney Int. 2015;87(1):20–30.
Adler AI, Stevens RJ, Manley SE, Bilous RW, Cull CA, Holman RR, et al. Development and progression of nephropathy in type 2 diabetes: the United Kingdom Prospective Diabetes Study (UKPDS 64). Kidney Int. 2003;63(1):225–32.
Bretzel RG. Prevention and slowing down the progression of the diabetic nephropathy through antihypertensive therapy. J Diabetes Complications. 1997;11(2):112–22.
Parving HH. Diabetic nephropathy: prevention and treatment. Kidney Int. 2001;60(5):2041–55.
Dasgupta I. Cost of treating diabetic kidney disease. Indian J Nephrol. 2014;24(3):139–40.
Strippoli GFM, Bonifati C, Craig M, Navaneethan SD, Craig JC. Angiotensin converting enzyme inhibitors and angiotensin II receptor antagonists for preventing the progression of diabetic kidney disease. Cochrane Database Syst Rev. 2006;(4):CD006257.
Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The Collaborative Study Group. N Engl J Med. 1993;329(20):1456–62.
Deerochanawong C, Kornthong P, Phongwiratchai S, Serirat S. Effects on urinary albumin excretion and renal function changes by delapril and manidipine in normotensive type 2 diabetic patients with microalbuminuria. J Med Assoc Thai. 2001;84(2):234–41.
Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med. 2001;345(12):861–9.
Novikov A, Vallon V. Sodium glucose cotransporter 2 inhibition in the diabetic kidney: an update: An update. CurrOpin Nephrol Hypertens. 2016;25(1):50–8.
Schork A, Saynisch J, Vosseler A, Jaghutriz BA, Heyne N, Peter A, et al. Effect of SGLT2 inhibitors on body composition, fluid status and renin-angiotensin-aldosterone system in type 2 diabetes: a prospective study using bioimpedance spectroscopy. Cardiovasc Diabetol. 2019;18(1):46.
Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644–57.
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–28.
Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–57.
Zhang X-L, Zhu Q-Q, Chen Y-H, Li X-L, Chen F, Huang J-A, et al. Cardiovascular safety, long-term noncardiovascular safety, and efficacy of sodium-glucose cotransporter 2 inhibitors in patients with type 2 diabetes mellitus: A systemic review and meta-analysis with trial sequential analysis. J Am Heart Assoc. 2018;7(2).
Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295–306.
Perkovic V, Jardine M, Vijapurkar U, Meininger G. Renal effects of canagliflozin in type 2 diabetes mellitus. Curr Med Res Opin. 2015;31(12):2219–31.
Hsia DS, Grove O, Cefalu WT. An update on sodium-glucose co-transporter-2 inhibitors for the treatment of diabetes mellitus. CurrOpin Endocrinol Diabetes Obes. 2017;24(1):73–9.
Khouri C, Cracowski J-L, Roustit M. SGLT-2 inhibitors and the risk of lower-limb amputation: Is this a class effect? Diabetes ObesMetab. 2018;20(6):1531–4.
Bersoff-Matcha SJ, Chamberlain C, Cao C, Kortepeter C, Chong WH. Fournier gangrene associated with sodium-glucose cotransporter-2 inhibitors: A review of spontaneous postmarketing cases. Ann Intern Med. 2019;170(11):764–9.
Heerspink HJL, Karasik A, Thuresson M, Melzer-Cohen C, Chodick G, Khunti K, et al. Kidney outcomes associated with use of SGLT2 inhibitors in real-world clinical practice (CVD-REAL 3): a multinational observational cohort study. Lancet Diabetes Endocrinol. 2020;8(1):27–35.
Kohan DE, Fioretto P, Tang W, List JF. Long-term study of patients with type 2 diabetes and moderate renal impairment shows that dapagliflozin reduces weight and blood pressure but does not improve glycemic control. Kidney Int. 2014;85(4):962–71.
Cherney DZI, Perkins BA, Soleymanlou N, Maione M, Lai V, Lee A, et al. Renal hemodynamic effect of sodium-glucose cotransporter 2 inhibition in patients with type 1 diabetes mellitus. Circulation. 2014;129(5):587–97.
Rossing P, Caramori ML, Chan JCN, Heerspink HJL, Hurst C, Khunti K, et al. KDIGO 2022 clinical practice guideline for diabetes management in chronic kidney disease. Kidney Int. 2022;102(5):S1–127.
