
Relationship Between Serum Uric Acid Levels and Kidney Allograft Function Within the First Year Post-Transplantation
Article Sidebar
Main Article Content
Abstract
Background: Hyperuricemia negatively impacts cardiovascular health in patients with chronic kidney disease and kidney transplant recipients. Lowering serum uric acid has been associated with improved outcomes following kidney transplantation. This study investigated the relationship between serum uric acid levels and kidney allograft function in transplant recipients.
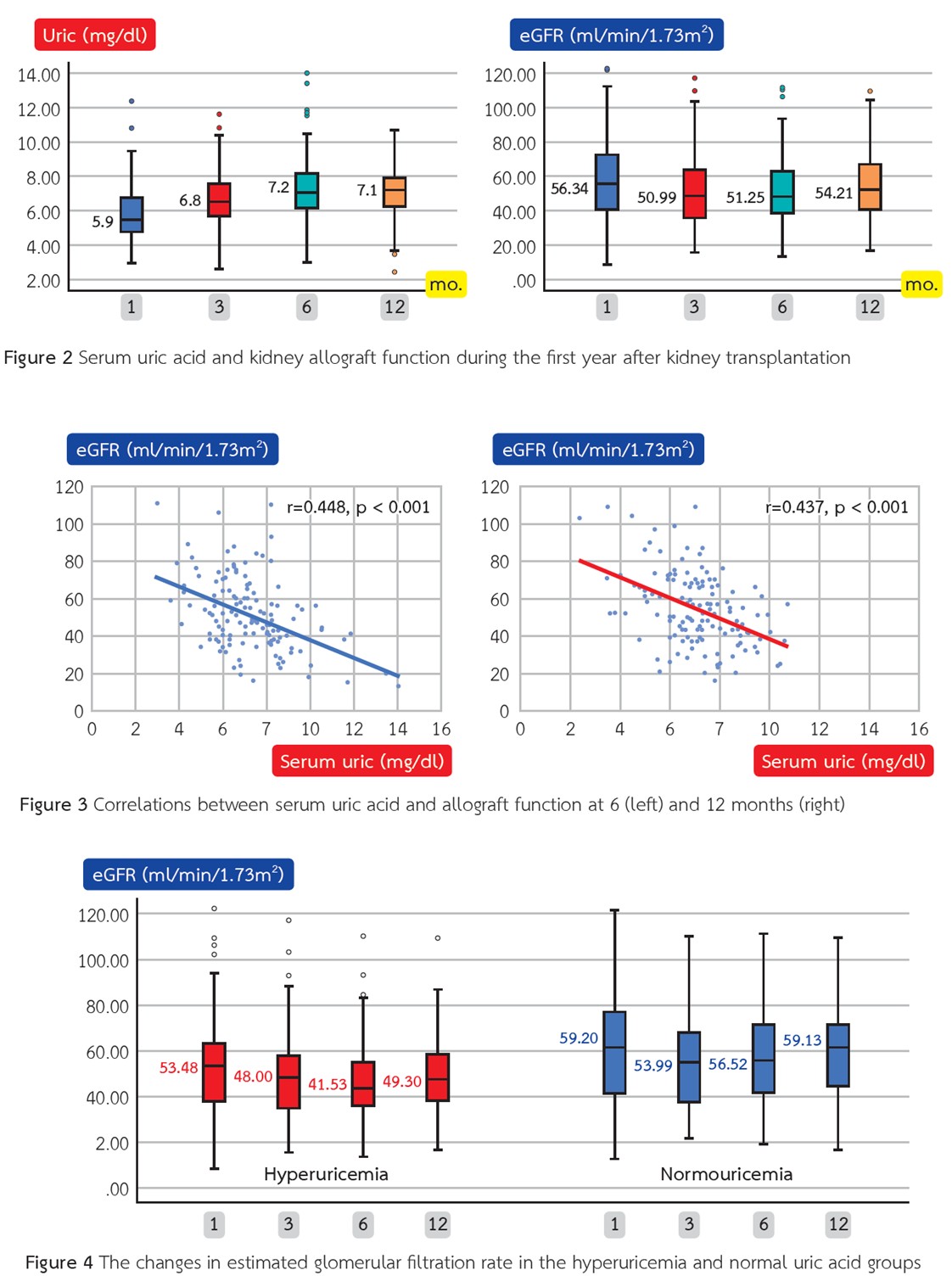
Methods: This retrospective, single-center cohort study included kidney transplant recipients within 12 months post-transplantation. Hyperuricemia was defined as a serum uric acid level greater than 7 mg/dL. The primary outcomes were the difference in allograft function between the hyperuricemia and normal uric acid group and the correlation between serum uric acid levels and kidney allograft function, measured by estimated glomerular filtration rate (eGFR) at 6 and 12 months post-transplant.
Results: A total of 134 patients were included in the study. By 6 months post-transplant, 50% of patients had developed hyperuricemia, with the majority being male. Serum uric acid levels were significantly and inversely correlated with eGFR at both 6 and 12 months. Although the hyperuricemia group showed a trend toward greater eGFR decline compared to the normal uric acid group, the between-group differences did not reach statistical significance. Nevertheless, eGFR values at both 6 and 12 months were substantially lower in the hyperuricemia group
Conclusions: The association between hyperuricemia and reduced kidney allograft function within the first year after transplantation was suggested. Further research is needed to determine whether elevated uric acid directly contributes to graft dysfunction or reflects declining kidney function.
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This article is published under CC BY-NC-ND 4.0 license, which allows for non-commercial reuse of the published paper as long as the published paper is fully attributed. Anyone can share (copy and redistribute) the material in any medium or format without having to ask permission from the author or the Nephrology Society of Thailand.
References
Mazali FC, Mazzali M. Uric acid and transplantation. Semin Nephrol 2011;31(5):466-71. doi: 10.1016/j.semnephrol. 2011.08.012.
Braga F, Pasqualetti S, Ferraro S, Panteghini M. Hyperuricemia as risk factor for coronary heart disease incidence and mortality in the general population: a systematic review and metaanalysis. Clin Chem Lab Med 2016;54(1):7-15. doi: 10.1515/cclm-2015-0523.
Kushiyama A, Nakatsu Y, Matsunaga Y, Yamamotoya T, Mori K, Ueda K, et al. Role of Uric Acid Metabolism-Related Inflammation in the Pathogenesis of Metabolic Syndrome Components Such as Atherosclerosis and Nonalcoholic Steatohepatitis. Mediators Inflamm 2016;2016:8603164. doi: 10.1155/2016/8603164.
Yang H, Chen Q, Huang A, Yu X, Chen G, Hu X, et al. The Impact of hyperuricemia on long-term clinical outcomes of renal transplant recipients: a systematic review and meta-analysis. J Pharm Pharm Sci 2021;24:292-307. doi: 10.18433/jpps31620.
Sotomayor CG, Oskooei SS, Bustos NI, Nolte IM, Gomes-Neto AW, Erazo M, et al. Serum uric acid is associated with increased risk of posttransplantation diabetes in kidney transplant recipients: a prospective cohort study. Metabolism 2021;116:154465. doi: 10.1016/j.metabol.2020.154465.
Tanaka K, Sakai K, Kushiyama A, Hara S, Hattori M, Ohashi Y, et al. Serum uric acid is an independent predictor of new-onset diabetes after living-donor kidney transplantation. Renal Replacement Therapy 2018;4(1):28. doi: 10.1186/s41100-018-0169-4.
Barkas F, Elisaf M, Liberopoulos E, Kalaitzidis R, Liamis G. Uric acid and incident chronic kidney disease in dyslipidemic individuals. Curr Med Res Opin 2018;34(7):1193-9. doi: 10.1080/03007995.2017.1372157.
Demirci B. Gurlek SS, Oygur C, Bal Z, Tutal E, Haberal M. Hyperuricemia Takes a Toll in Graft Function, Left Ventricular Diameters and Arterial Stiffness in Renal Transplant Recipients. Am J Transplant 2015;15.
Erkmen Uyar M, Sezer S, Bal Z, Guliyev O, Tutal E, Kulah E, et al. Post-transplant Hyperuricemıa as a Cardıovascular Risk Factor. Transplant Proc 2015;47(4):1146-51. doi: 10.1016/j.transproceed.2015.03.004.
Clive DM. Renal transplant-associated hyperuricemia and gout. J Am Soc Nephrol 2000;11(5):974-9. doi: 10.1681/asn.V115974.
Halperin Kuhns VL, Woodward OM. Sex Differences in Urate Handling. Int J Mol Sci 2020;21(12). doi: 10.3390/ijms21124269.
Cheng M, Pérez RE, Santiago JC, Galindo AC, Carreño Rodríguez YR, Guerrero Rosario AO, et al. Complications of Renal Transplantation That Influence the Presence of Hyperuricemia in Its First Year of Evolution. Transplant Proc 2020;52(4):1147-51. doi: 10.1016/j.transproceed.2020.01.062.
Johnson RJ, Kivlighn SD, Kim YG, Suga S, Fogo AB. Reappraisal of the pathogenesis and consequences of hyperuricemia in hypertension, cardiovascular disease, and renal disease. Am J Kidney Dis 1999;33(2):225-34. doi: 10.1016/s0272-6386(99)70295-7.
Kim DG, Kim BS, Choi HY, Lim BJ, Huh KH, Kim MS, et al. Association between post-transplant uric acid level and renal allograft fibrosis: Analysis using Banff pathologic scores from renal biopsies. Sci Rep 2018;8(1):11601. doi: 10.1038/s41598-018-29948-9.
Einollahi B, Einollahi H, Nafar M, Rostami Z. Prevalence and risk factors of hyperuricemia among kidney transplant recipients. Indian J Nephrol 2013;23(3):201-5. doi: 10.4103/0971-4065.111849.
Marcén R, Gallego N, Orofino L, Gámez C, Estepa MR, Sabater J, et al. Impairment of tubular secretion of urate in renal transplant patients on cyclosporine. Nephron 1995;70(3):307-13. doi: 10.1159/000188609.
Steidel K, Brandis M, Kramer M, Leititis JU, Zimmerhackl LB. Cyclosporine inhibits renal uric acid transport in renal transplants not in children treated for nephrotic syndrome. Ren Fail 1990;12(3):193-8. doi: 10.3109/08860229009065563.
