
ความสัมพันธ์ระหว่างระดับกรดยูริกในเลือดกับการทำงานของไตที่ปลูกถ่ายช่วงหนึ่งปีแรก หลังการปลูกถ่ายไต
Article Sidebar
Main Article Content
บทคัดย่อ
บทนำ: ภาวะกรดยูริกในเลือดสูง (Hyperuricemia) ส่งผลเสียต่อสุขภาพหัวใจและหลอดเลือดในผู้ป่วยโรคไตเรื้อรังและผู้ที่ได้รับการปลูกถ่ายไต การลดระดับกรดยูริกในเลือดมีความเกี่ยวข้องกับผลลัพธ์ที่ดีขึ้นหลังการปลูกถ่ายไต งานวิจัยนี้ศึกษาความสัมพันธ์ระหว่างระดับกรดยูริกในเลือดกับการทำงานของไตที่ปลูกถ่ายในผู้รับการปลูกถ่ายไต
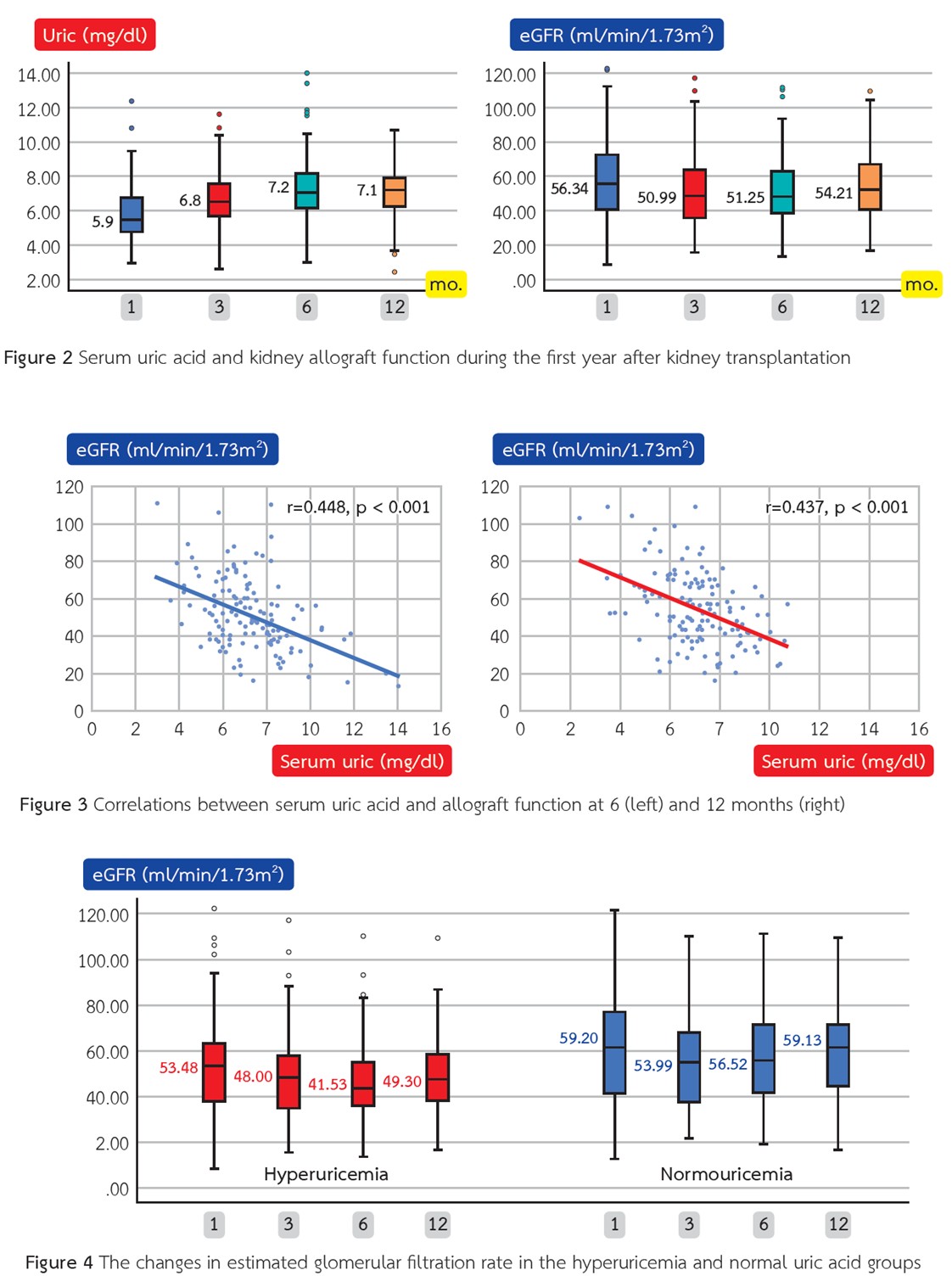
ระเบียบวิธีวิจัย: การศึกษาเชิงย้อนหลังแบบกลุ่มตัวอย่างในศูนย์เดียว โดยรวบรวมข้อมูลจากผู้ป่วยปลูกถ่ายไตที่มีระยะเวลาหลังการปลูกถ่ายไม่เกิน 12 เดือน กำหนดภาวะกรดยูริกในเลือดสูงว่าเป็นระดับกรดยูริกในเลือดมากกว่า 7 มก./ดล. ผลลัพธ์หลักที่ศึกษา คือ ความแตกต่างของการทำงานของไตที่ปลูกถ่ายระหว่างกลุ่มที่มีกรดยูริกในเลือดสูงกับกลุ่มที่มีกรดยูริกในเลือดปกติ และความสัมพันธ์ระหว่างระดับกรดยูริกในเลือดกับการทำงานของไตที่ปลูกถ่าย ซึ่งประเมินจากอัตราการกรองของไตโดยประมาณ (eGFR) ที่ 6 และ 12 เดือนหลังการปลูกถ่าย
ผลการวิจัย: มีผู้ป่วยรวมทั้งสิ้น 134 รายเข้าร่วมการศึกษา โดยภายใน 6 เดือนหลังการปลูกถ่าย พบว่าร้อยละ 50 ของผู้ป่วยมีภาวะกรดยูริกในเลือดสูง และส่วนใหญ่เป็นเพศชาย ระดับกรดยูริกในเลือดมีความสัมพันธ์ทางลบอย่างมีนัยสำคัญกับค่า eGFR ทั้งในช่วง 6 และ 12 เดือน แม้ว่ากลุ่มที่มีภาวะกรดยูริกในเลือดสูงจะแสดงแนวโน้มของการลดลงของ eGFR มากกว่ากลุ่มที่มีกรดยูริกในเลือดปกติ แต่ความแตกต่างระหว่างกลุ่มไม่ถึงระดับนัยสำคัญทางสถิติ อย่างไรก็ตาม ค่า eGFR ทั้งในช่วง 6 และ 12 เดือนในกลุ่มกรดยูริกในเลือดสูง ต่ำกว่ากลุ่มกรดยูริกในเลือดปกติอย่างมีนัยสำคัญ
สรุป: การศึกษานี้ชี้ให้เห็นถึงความสัมพันธ์ระหว่างภาวะกรดยูริกในเลือดสูงกับการทำงานของไตที่ปลูกถ่ายที่ลดลงภายในหนึ่งปีหลังการปลูกถ่าย อย่างไรก็ตามยังจำเป็นต้องมีการวิจัยเพิ่มเติมเพื่อระบุว่า ระดับกรดยูริกที่สูงส่งผลต่อการเสื่อมของไตที่ปลูกถ่ายโดยตรง หรือเป็นเพียงผลลัพธ์จากการทำงานของไตที่ลดลง
Article Details

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
บทความนี้ตีพิมพ์ภายไต้การอนุญาต CC BY-NC-ND 4.0 ซึ่งอนุญาตให้สามารถใช้บทความนี้พื่อวัตถุประสงค์ใดๆ ก็ตามที่ไม่ใช่เชิงพาณิชย์ โดยต้องมีการอ้างถึงที่มาของบทความอย่างครบถ้วน ใครก็ตามสามารถคัดลอกและแจกจ่ายทุกส่วนของบทความนี้โดยไม่ต้องขออนุญาตจากผู้ประพันธ์หรือสมาคมโรคไตแห่งประเทศไทย
เอกสารอ้างอิง
Mazali FC, Mazzali M. Uric acid and transplantation. Semin Nephrol 2011;31(5):466-71. doi: 10.1016/j.semnephrol. 2011.08.012.
Braga F, Pasqualetti S, Ferraro S, Panteghini M. Hyperuricemia as risk factor for coronary heart disease incidence and mortality in the general population: a systematic review and metaanalysis. Clin Chem Lab Med 2016;54(1):7-15. doi: 10.1515/cclm-2015-0523.
Kushiyama A, Nakatsu Y, Matsunaga Y, Yamamotoya T, Mori K, Ueda K, et al. Role of Uric Acid Metabolism-Related Inflammation in the Pathogenesis of Metabolic Syndrome Components Such as Atherosclerosis and Nonalcoholic Steatohepatitis. Mediators Inflamm 2016;2016:8603164. doi: 10.1155/2016/8603164.
Yang H, Chen Q, Huang A, Yu X, Chen G, Hu X, et al. The Impact of hyperuricemia on long-term clinical outcomes of renal transplant recipients: a systematic review and meta-analysis. J Pharm Pharm Sci 2021;24:292-307. doi: 10.18433/jpps31620.
Sotomayor CG, Oskooei SS, Bustos NI, Nolte IM, Gomes-Neto AW, Erazo M, et al. Serum uric acid is associated with increased risk of posttransplantation diabetes in kidney transplant recipients: a prospective cohort study. Metabolism 2021;116:154465. doi: 10.1016/j.metabol.2020.154465.
Tanaka K, Sakai K, Kushiyama A, Hara S, Hattori M, Ohashi Y, et al. Serum uric acid is an independent predictor of new-onset diabetes after living-donor kidney transplantation. Renal Replacement Therapy 2018;4(1):28. doi: 10.1186/s41100-018-0169-4.
Barkas F, Elisaf M, Liberopoulos E, Kalaitzidis R, Liamis G. Uric acid and incident chronic kidney disease in dyslipidemic individuals. Curr Med Res Opin 2018;34(7):1193-9. doi: 10.1080/03007995.2017.1372157.
Demirci B. Gurlek SS, Oygur C, Bal Z, Tutal E, Haberal M. Hyperuricemia Takes a Toll in Graft Function, Left Ventricular Diameters and Arterial Stiffness in Renal Transplant Recipients. Am J Transplant 2015;15.
Erkmen Uyar M, Sezer S, Bal Z, Guliyev O, Tutal E, Kulah E, et al. Post-transplant Hyperuricemıa as a Cardıovascular Risk Factor. Transplant Proc 2015;47(4):1146-51. doi: 10.1016/j.transproceed.2015.03.004.
Clive DM. Renal transplant-associated hyperuricemia and gout. J Am Soc Nephrol 2000;11(5):974-9. doi: 10.1681/asn.V115974.
Halperin Kuhns VL, Woodward OM. Sex Differences in Urate Handling. Int J Mol Sci 2020;21(12). doi: 10.3390/ijms21124269.
Cheng M, Pérez RE, Santiago JC, Galindo AC, Carreño Rodríguez YR, Guerrero Rosario AO, et al. Complications of Renal Transplantation That Influence the Presence of Hyperuricemia in Its First Year of Evolution. Transplant Proc 2020;52(4):1147-51. doi: 10.1016/j.transproceed.2020.01.062.
Johnson RJ, Kivlighn SD, Kim YG, Suga S, Fogo AB. Reappraisal of the pathogenesis and consequences of hyperuricemia in hypertension, cardiovascular disease, and renal disease. Am J Kidney Dis 1999;33(2):225-34. doi: 10.1016/s0272-6386(99)70295-7.
Kim DG, Kim BS, Choi HY, Lim BJ, Huh KH, Kim MS, et al. Association between post-transplant uric acid level and renal allograft fibrosis: Analysis using Banff pathologic scores from renal biopsies. Sci Rep 2018;8(1):11601. doi: 10.1038/s41598-018-29948-9.
Einollahi B, Einollahi H, Nafar M, Rostami Z. Prevalence and risk factors of hyperuricemia among kidney transplant recipients. Indian J Nephrol 2013;23(3):201-5. doi: 10.4103/0971-4065.111849.
Marcén R, Gallego N, Orofino L, Gámez C, Estepa MR, Sabater J, et al. Impairment of tubular secretion of urate in renal transplant patients on cyclosporine. Nephron 1995;70(3):307-13. doi: 10.1159/000188609.
Steidel K, Brandis M, Kramer M, Leititis JU, Zimmerhackl LB. Cyclosporine inhibits renal uric acid transport in renal transplants not in children treated for nephrotic syndrome. Ren Fail 1990;12(3):193-8. doi: 10.3109/08860229009065563.
