ปัจจัยที่เกี่ยวข้องกับระยะเวลานอนโรงพยาบาลของผู้ป่วย หลังการผ่าตัดลำไส้อุดตันในเขตเมือง
คำสำคัญ:
ระยะเวลานอนโรงพยาบาล, ลำไส้อุดตัน, เขตเมืองบทคัดย่อ
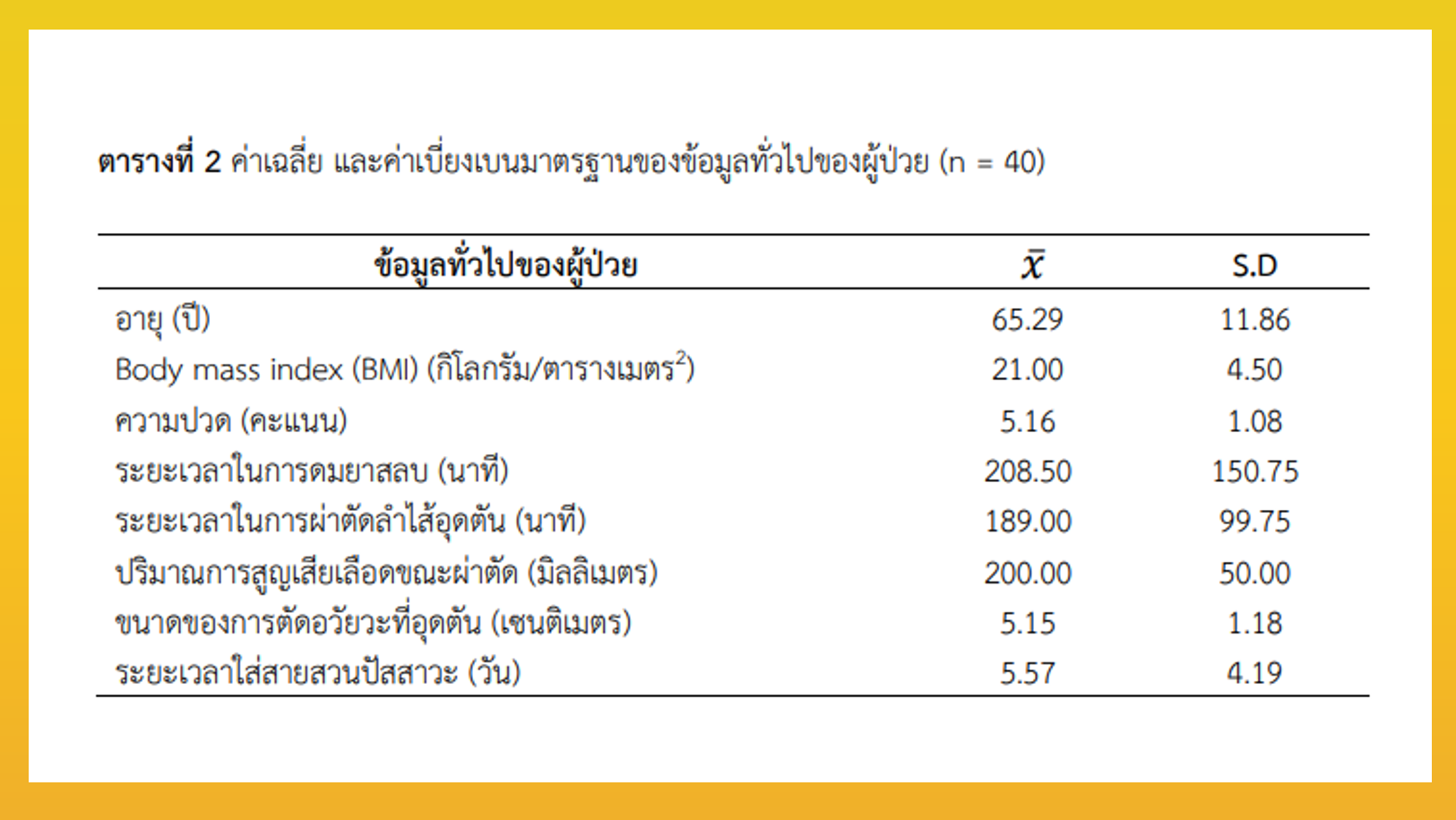
การวิจัยเชิงพรรณนาแบบย้อนหลังนี้ มีวัตถุประสงค์เพื่อศึกษาปัจจัยที่เกี่ยวข้องกับระยะเวลานอนโรงพยาบาลของผู้ป่วยหลังการผ่าตัดลำไส้อุดตันในเขตเมือง กลุ่มตัวอย่าง คือ ผู้ป่วยที่อาศัยในเขตเมือง และได้รับการผ่าตัดลำไส้อุดตัน เข้ารับการรักษาที่คณะแพทยศาสตร์วชิรพยาบาล โดยเก็บข้อมูลจากเวชระเบียน ระหว่างวันที่ 1 มกราคม ถึงวันที่ 31 ธันวาคม พ.ศ. 2563 รวม 40 ราย เครื่องมือวิจัยประกอบด้วย 2 ส่วน คือ 1) ข้อมูลทั่วไป และ 2) ข้อมูลเกี่ยวกับประวัติการรักษา แบบบันทึกข้อมูลผ่านการตรวจความตรงทางเนื้อหา และความเที่ยงตรงเชิงเนื้อหาด้วยดัชนีความสอดคล้องรายข้อ อยู่ในช่วง .70 - .80 วิเคราะห์ข้อมูลด้วยสถิติเชิงพรรณนา และวิเคราะห์ความสัมพันธ์ของปัจจัยด้วยสหสัมพันธ์ของสเปียร์แมน สัมประสิทธิ์ฟี และฟิชเชอร์
ผลการวิจัย พบว่า ปัจจัยในระยะก่อนการผ่าตัด และระยะขณะทำการผ่าตัดลำไส้อุดตันไม่มีความสัมพันธ์กับระยะเวลานอนโรงพยาบาล ปัจจัยระยะหลังการผ่าตัด พบว่า ระยะเวลาการใส่สายไว้ในร่างกาย ได้แก่ ระยะเวลาใส่สายให้สารน้ำทางหลอดเลือดดำ (r = .595, p-value < .001) ระยะเวลาใส่สายสวนปัสสาวะ (r = .533, p-value < .001) มีความสัมพันธ์กับระยะเวลานอนโรงพยาบาลไปในทิศทางเดียวกันอย่างมีนัยสำคัญทางสถิติ
สรุปได้ว่า การให้ความสำคัญในการกระตุ้นการฟื้นหายหลังการผ่าตัด เป็นปัจจัยสำคัญที่อาจจะช่วยลดระยะเวลานอนโรงพยาบาลของผู้ป่วยหลังการผ่าตัดลำไส้อุดตันในเขตเมืองได้
เอกสารอ้างอิง
Ministry of Public Health. Public health statistics 2019 [Internet]. 2019 [cited 10 Oct 2020]. Available from: https://dmsic.moph.go.th/index/detail/8297 (in Thai)
Andersen K, Thastum M, Nørholt SE, Blomlöf J. Relative blood loss and operative time can predict length of stay following orthognathic surgery. International Journal of Oral and Maxillofacil Surgery 2016;45(10):1209-12. doi: 10.1016/j.ijom.2016.05.015.
Griffiths S, Glancy DG. Intestinal obstruction. Surgery (Oxford) 2020;38(1):43-50. doi: 10.1016/j.mpsur.2019.10.014.
Catena F, De Simone B, Coccolini F, Di Saverio S, Sartelli M, Ansaloni L. Bowel obstruction: a narrative review for all physicians. World Journal of Emergency Surgery 2019;14:20. doi: 10.1186/s13017-019-0240-7.
Abdellatef H, Yousef A, Khater H, Abdel RA. Role of multi detector CT in diagnosis of small and large bowel obstruction. Benha Medical Journal 2021;38 Suppl 1:22-33. doi: 10.21608/bmfj.2021.141670.
Sakari T, Christersson M, Karlbom U. Mechanisms of adhesive small bowel obstruction and outcome of surgery; a population-based study. BMC Surgery 2020;20(1):62. doi: 10.1186/s12893-020-00724-9.
Russell T, Chen F. Quality issues in emergency colorectal surgery. Seminars in Colon and Rectal Surgery 2020;31(4):100784. doi: 10.1016/j.scrs.2020.100784.
Mehdorn M, Groos L, Kassahun W, Jansen-Winkeln B, Gockel I, Moulla Y. Interrupted sutures prevent recurrent abdominal fascial dehiscence: a comparative retrospective single center cohort analysis of risk factors of burst abdomen and its recurrence as well as surgical repair techniques. BMC Surgery 2021;21(1):208. doi: 10.1186/s12893-021-01219-x.
Afshari K, Smedh K, Wagner P, Chabok A, Nikberg M. Risk factors for developing anorectal dysfunction after anterior resection. International Journal of Colorectal Disease 2021;36(12):2697-705. doi: 10.1007/s00384-021-04024-3.
Van der Kuur A, Bethlehem C, Bruins N, de Jager C, van Alst C, Haagsma OG, et al. Impact of a premorbid psychiatric disorder on the incidence of delirium during ICU stay, morbidity, and long-term mortality. Crital Care Research and Practice 2019;2019:6402097. doi: 10.1155/2019/6402097.
Krejcie RV, Morgan DW. Determining sample size for research activities. Educational and Psychological Measurement 1970;30:607-10. doi: 10.1177/001316447003000308.
Zhou C, Wu XR, Liu XH, Chen YF, Ke J, He XS, et al. Male gender is associated with anincreased risk of anastomotic leak in rectal cancer patients after total mesorectal excision. Gastroenterology Report 2018;6(2):137-43. doi: 10.1093/gastro/gox039.
Salma RG, Shammari FM, Garni BA, Qarzaee MA. Operative time, blood loss, hemoglobin drop, blood transfusion, and hospital stay in orthognathic surgery. Maxillofacial Surgery 2017;21(2):259-66. doi: 10.1007/s10006-017-0626-1.
Surkan MJ, Gibson W. Interventions to mobilize elderly patients and reduce length of hospital stay. Canadian Journal Cardiology 2018;34(7):881-8. doi: 10.1016/j.cjca.2018.04.033.
Miller TE, Roche AM, Mythen M. Fluid management and goal-directed therapy as an adjunct to enhanced recovery after surgery (ERAS). Canadian Journal of Anaesthesia 2015;62(2):158-68. doi: 10.1007/s12630-014-0266-y.
Arteaga M, Ramírez B, Rodríguez SJ. The effects of prone position ventilation in patients with acute respiratory distress syndrome. A systematic review and metaanalysis. Intensive Care Medicine 2015;39(6):359-72. doi: 10.1016/j.medine.2014.11.004.
Lohsiriwat V, Jitmungngan R. Enhanced recovery after surgery in emergency colorectal surgery: review of literature and current practices. World Journal of Gastrointestinal Surgery 2019;11(2):41-52. doi: 10.4240/wjgs.v11.i2.41.
Jakobson T, Karjagin J, Vipp L, Padar M, Parik AH, Starkopf L, et al. Postoperative complications and mortality after major gastrointestinal surgery. Medicina (Kaunas) 2014;50(2):111-7.doi: 10.1016/j.medici.2014.06.002.
Sharma J, Kumar N, Huda F, Payal YS. Enhanced recovery after surgery protocol in emergency laparotomy: a randomized control study. The Surgery Journal 2021;7(2):e92-9. doi: 10.1055/s-0041-1725156.
Katsuki R, Jo T, Yasunaga H, Ishimaru M, Sakamoto T. Outcomes of self-expandable metal stent as bridge to surgery versus emergency surgery for left-sided obstructing colon cancer: a retrospective cohort study. American Journal of Surgery 2021;221(1):168-73. doi: 10.1016/j.amjsurg.2020.06.012.
ดาวน์โหลด
เผยแพร่แล้ว
รูปแบบการอ้างอิง
ฉบับ
ประเภทบทความ
สัญญาอนุญาต
ลิขสิทธิ์ (c) 2023 วารสารเกื้อการุณย์

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.