
ปัจจัยที่มีความสัมพันธ์กับการไม่ฟื้นตัวของไตในผู้ป่วยภาวะไตวายเฉียบพลันจากภาวะติดเชื้อ
Article Sidebar
Main Article Content
บทคัดย่อ
บทนำ: ภาวะไตวายเฉียบพลันที่มีสาเหตุมาจาการติดเชื้อหรือการติด เชื้อในกระแสเลือด เป็นภาวะแทรกซ้อนที่พบได้บ่อยในผู้ป่วยที่นอนในโรงพยาบาล ส่งผลต่ออัตราการตายที่เพิ่มขึ้นรวมไปถึงอัตราการครองเตียง ปัจจุบันมีการศึกษาจำนวนน้อยที่สนใจปัจจัยที่ส่งผลต่อการฟื้นตัวของไตหลังการเกิดภาวะไตวายเฉียบพลัน
ระเบียบวิธีวิจัย: การศึกษานี้เป็นการเก็บข้อมูลย้อนหลังของผู้ป่วยที่เข้า รับการรักษาในโรงพยาบาลด้วยภาวะไตวายเฉียบพลันที่มีสาเหตุมาจากการติดเชื้อ ระหว่างวันที่ 1 มกราคม พ.ศ. 2558 ถึงวันที่ 31 ธันวาคม พ.ศ. 2563 โดยผู้ป่วยจะได้รับการแบ่งออกเป็น 2 กลุ่ม คือ กลุ่มที่มีการฟื้นตัวของไตอย่างสมบูรณ์ และกลุ่มที่ไม่มีการฟื้นตัวของไต จากนั้นจะ ทำการวิเคราะห์ปัจจัยที่มีความสัมพันธ์กับการไม่ฟื้นตัวของไตภายในระยะเวลา 90 วัน
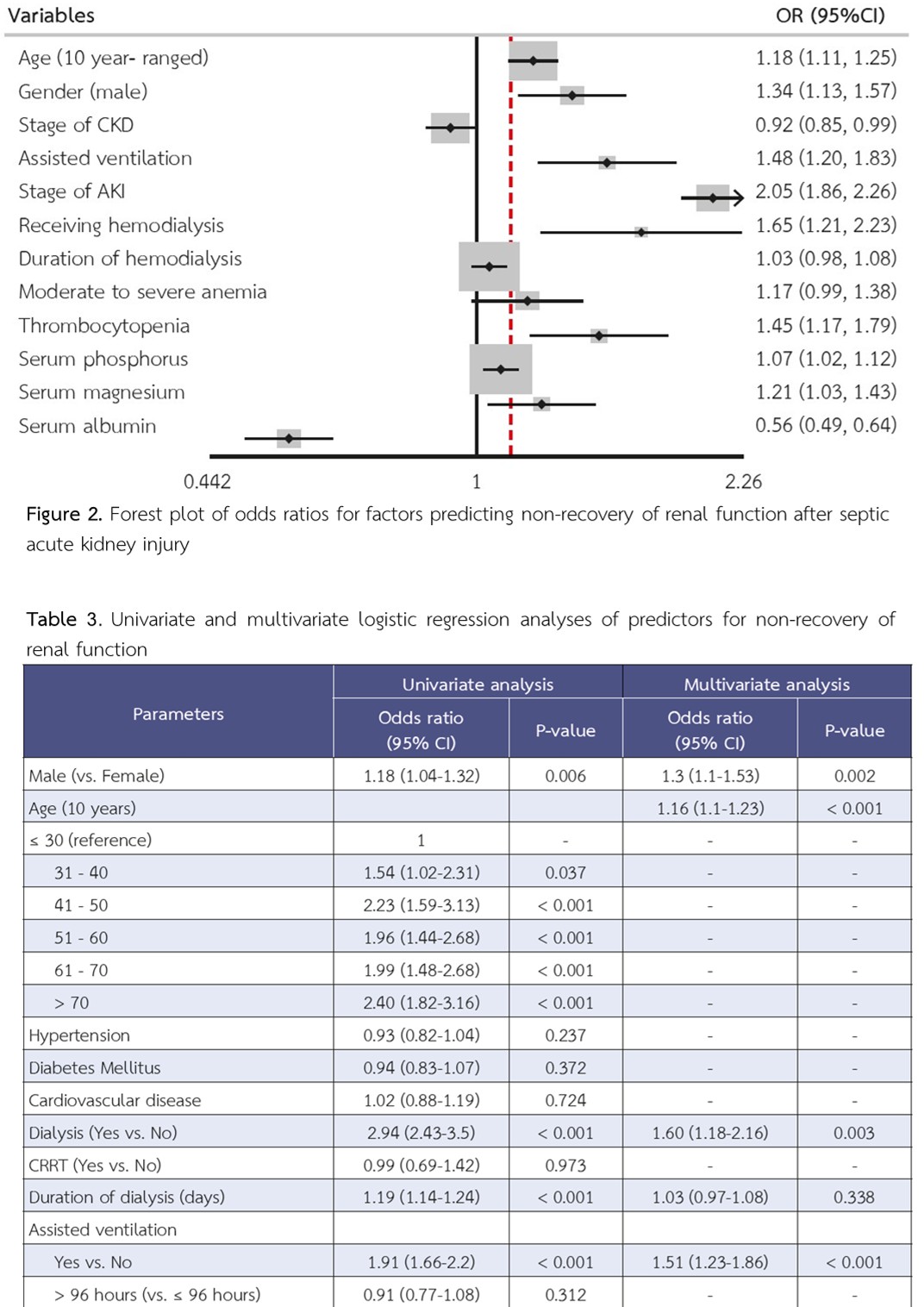
ผลการวิจัย: มีผู้ป่วยที่ผ่านเกณฑ์การคัดเข้าและออกทั้งหมด จำนวน 4431 คน ในจำนวนนี้ผู้ป่วย 2,429 ราย (ร้อยละ 54.82) มีการฟื้นตัวของ ไตอย่างสมบูรณ์ และ 2,002 ราย (ร้อยละ 45.18) ไม่มีการฟื้นตัวของไต จากการวิเคราะห์แบบพหุตัวแปร ปัจจัยที่พบว่ามีความสัมพันธ์กับการไม่ฟื้นตัวของไต ได้แก่ อายุที่เพิ่มขึ้น เพศชาย ความรุนแรงของภาวะไตวายเฉียบพลัน การได้รับการบำบัดทดแทนไต การใช้เครื่องช่วยหายใจ ภาวะเกร็ดเลือดต่ำ ระดับฟอสฟอรัส และแมกนีเซียมที่เพิ่มขึ้น และระดับอัลบูมินในเลือดที่ลดลง ทั้งนี้ไม่พบความสัมพันธ์ระหว่างโรคประจำตัวและความรุนแรงของโรคไตเรื้อรังกับผลลัพธ์ทางไต
สรุป: ปัจจัยที่มีความสัมพันธ์กับการไม่ฟื้นตัวของไตหลังการเกิดภาวะ ไตวายเฉียบพลันที่มีสาเหตุจากการติดเชื้อ ได้แก่ อายุที่เพิ่มขึ้น เพศชาย ความรุนแรงของไตวายเฉียบพลัน การได้รับการบำบัดทดแทนไต การใช้เครื่องช่วยหายใจ เกร็ดเลือดและระดับอัลบูมินในเลือดต่ำ
Article Details

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
บทความนี้ตีพิมพ์ภายไต้การอนุญาต CC BY-NC-ND 4.0 ซึ่งอนุญาตให้สามารถใช้บทความนี้พื่อวัตถุประสงค์ใดๆ ก็ตามที่ไม่ใช่เชิงพาณิชย์ โดยต้องมีการอ้างถึงที่มาของบทความอย่างครบถ้วน ใครก็ตามสามารถคัดลอกและแจกจ่ายทุกส่วนของบทความนี้โดยไม่ต้องขออนุญาตจากผู้ประพันธ์หรือสมาคมโรคไตแห่งประเทศไทย
เอกสารอ้างอิง
Hoste EAJ, Bagshaw SM, Bellomo R, Cely CM, Colman R, Cruz DN, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 2015;41(8):1411–23.
Motzkus CA, Chrysanthopoulou SA, Luckmann R, Rincon TA, Lapane KL, Lilly CM. ICU Admission Source as a Predictor of Mortality for Patients With Sepsis. J Intensive Care Med. 2018;33(9):510–6.
Bagshaw SM, Uchino S, Bellomo R, Morimatsu H, Morgera S, Schetz M, et al. Septic Acute Kidney Injury in Critically Ill Patients: Clinical Characteristics and Outcomes. Clin J Am Soc Nephrol. 2007;2(3):431–9.
Palevsky PM, Molitoris BA, Okusa MD, Levin A, Waikar SS, Wald R, et al. Design of Clinical Trials in Acute Kidney Injury: Report from an NIDDK Workshop on Trial Methodology. Clin J Am Soc Nephrol. 2012;7(5):844–50.
Khwaja A. KDIGO Clinical Practice Guidelines for Acute Kidney Injury. Nephron. 2012;120(4):c179–84.
Goldstein SL, Chawla L, Ronco C, Kellum JA. Renal recovery. Crit Care. 2014;18(1):301. doi: 10.1186/cc13180.
Chawla LS, Eggers PW, Star RA, Kimmel PL. Acute Kidney Injury and Chronic Kidney Disease as Interconnected Syndromes. N Engl J Med. 2014;371(1):58–66.
Kellum JA. How Can We Define Recovery after Acute Kidney Injury? Considerations from Epidemiology and Clinical Trial Design. Nephron Clin Pract. 2014;127(1–4):81–8.
Hsu C, Hsu RK, Yang J, Ordonez JD, Zheng S, Go AS. Elevated BP after AKI. J Am Soc Nephrol. 2016;27(3):914–23.
Go AS, Hsu C, Yang J, Tan TC, Zheng S, Ordonez JD, et al. Acute Kidney Injury and Risk of Heart Failure and Atherosclerotic Events. Clin J Am Soc Nephrol. 2018;13(6):833–41.
Legrand M, Rossignol P. Cardiovascular Consequences of Acute Kidney Injury. Ingelfinger JR, editor. N Engl J Med. 2020;382(23):2238–47.
Fiorentino M, Tohme FA, Wang S, Murugan R, Angus DC, Kellum JA. Long-term survival in patients with septic acute kidney injury is strongly influenced by renal recovery. Ricci Z, editor. PLoS ONE. 2018;13(6):e0198269. doi: 10.1371/journal. pone.0198269.
Kellum JA, Chawla LS, Keener C, Singbartl K, Palevsky PM, Pike FL, et al. The Effects of Alternative Resuscitation Strategies on Acute Kidney Injury in Patients with Septic Shock. Am J Respir Crit Care Med. 2016;193(3):281–7.
Sood MM, Shafer LA, Ho J, Reslerova M, Martinka G, Keenan S, et al. Early reversible acute kidney injury is associated with improved survival in septic shock. J Crit Care. 2014;29(5):711–7.
Chen JCY, Hu B, Frank RD, Kashani KB. Inpatient Kidney Function Recovery among Septic Shock Patients Who Initiated Kidney Replacement Therapy in the Hospital. Nephron. 2020;144(8):363–71.
Sukmark T, Lumlertgul N, Praditpornsilpa K, Tungsanga K, Eiam-Ong S, Srisawat N. SEA-MAKE score as a tool for predicting major adverse kidney events in critically ill patients with acute kidney injury: results from the SEA-AKI study. Ann Intensive Care. 2020;10(1):42. doi: 10.1186/s13613-020-00657-9.
Alobaidi R, Basu RK, Goldstein SL, Bagshaw SM. Sepsis-Associated Acute Kidney Injury. Semin Nephrol. 2015;35(1):2–11.
Pannu N, James M, Hemmelgarn B, Klarenbach S, for the Alberta Kidney Disease Network. Association between AKI, Recovery of Renal Function, and Long-Term Outcomes after Hospital Discharge. Clin J Am Soc Nephrol. 2013;8(2):194–202.
de Boer IH, Caramori ML, Chan JCN, Heerspink HJL, Hurst C, Khunti K, et al. KDIGO 2020 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int. 2020;98(4):S1–115.
Kellum JA, Sileanu FE, Bihorac A, Hoste EAJ, Chawla LS. Recovery after Acute Kidney Injury. Am J Respir Crit Care Med. 2017;195(6):784–91.
Forni LG, Darmon M, Ostermann M, Oudemans-van Straaten HM, Pettilä V, Prowle JR, et al. Renal recovery after acute kidney injury. Intensive Care Med. 2017;43(6):855–66.
Herrmann FR. Serum Albumin Level on Admission as a Predictor of Death, Length of Stay, and Readmission. Arch Intern Med. 1992;152(1):125-30.
Lee C-W, Kou H, Chou H-S, Chou H, Huang S-F, Chang C-H, et al. A combination of SOFA score and biomarkers gives a better prediction of septic AKI and in-hospital mortality in critically ill surgical patients: a pilot study. World J Emerg Surg. 2018;13(1):41. doi: 10.1186/s13017-018-0202-5.
