
Sodium-Glucose Cotransporter 2 Inhibitors ในภาวะไตวายเฉียบพลัน
Article Sidebar
Main Article Content
บทคัดย่อ
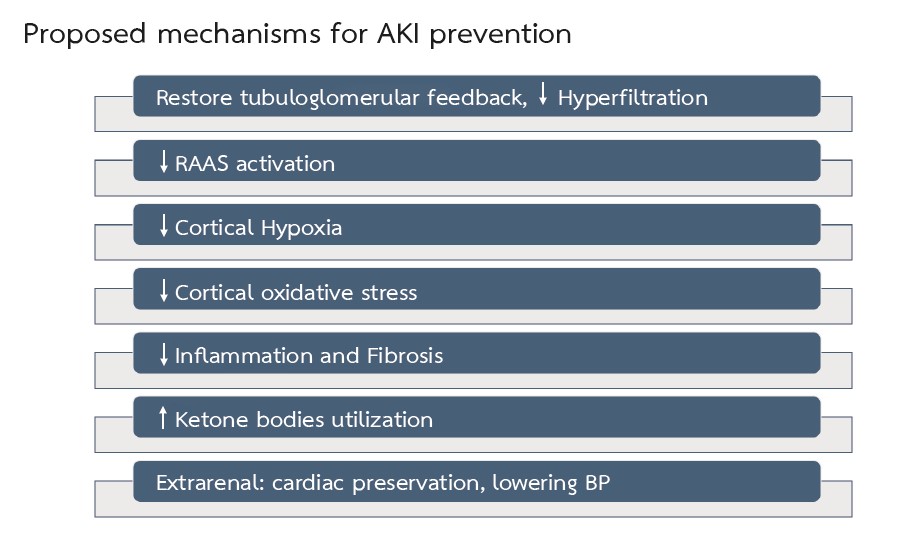
ภาวะไตวายเฉียบพลันพบได้บ่อยในผู้ป่วยที่นอนในโรงพยาบาล และภาวะไตวายเฉียบพลันสามารถเพิ่มความเสี่ยงต่อการเจ็บป่วยและการเสียชีวิต นอกจากนี้ผู้ป่วยที่มีประวัติของภาวะไตวายเฉียบพลันมีความเสี่ยงเพิ่มขึ้นต่อการเกิดโรคหัวใจและหลอดเลือดการนอนโรงพยาบาลซ้ำ การกลับมาของภาวะไตวายเฉียบพลัน การการเกิดโรคไตเรื้อรัง และการเกิดโรคไตเรื้อรังระยะสุดท้าย ณ ปัจจุบัน ยังไม่มีการรักษาที่จำเพาะสำหรับผู้ป่วยที่มีภาวะไตวายเฉียบพลัน ยาที่มีฤทธิ์ยับยั้งการทำงานของ Sodium-Glucose Cotransporter 2 (SGLT2 inhibitors) เป็นยา กลุ่มใหม่ที่มีการใช้อย่างแพร่หลายในระยะ 5 ปีที่ผ่านมา เพื่อวัตถุประสงค์ในการควบคุมระดับน้ำตาลในเลือด ชะลอการเสื่อมของไตและลดการเกิดผลลัพธ์ที่ไม่ดีของหัวใจและหลอดเลือด ยา SGLT2 inhibitors ออกฤทธิ์โดยไปยับยั้งการทำงานของ SGLT2 ที่ proximal tubules ส่งผลให้เกิดการขับน้ำตาลและโซเดียมออกทางปัสสาวะ ซึ่งนอกจากจะช่วยลดระดับน้ำตาลในเลือดแล้วยังช่วยเพิ่มการขับน้ำ ลดการคั่งของน้ำภายในระบบไหลเวียน และภายในช่องระหว่างเซลล์ (interstitium) และลดการทำงานของระบบประสาทซิมพาเทติก ยา SGLT2 inhibitors สามารถลด oxidative stress และภาวะการอักเสบในหัวใจ ซึ่งช่วยในการป้องกันการบาดเจ็บของหัวใจ การยับยั้งการทำงานของ Na+/H+ exchanger ในเซลล์กล้ามเนื้อหัวใจยังสามารถช่วยลดการเกิดภาวะหัวใจล้มเหลวได้อีกด้วย สำหรับในไตนั้นจากการศึกษาพบว่า SGLT2 inhibitors สามารถลดความต้องการและการใช้ออกซิเจนในบริเวณ renal cortex ถึงแม้ว่าในปัจจุบันจะยังไม่มีการศึกษาโดยตรงถึงประสิทธิภาพของ SGLT2 inhibitors ในการป้องกันภาวะไตวายเฉียบพลัน แต่กลไกการออกฤทธิ์เหล่านี้เป็นหลักฐานทางอ้อมที่น่าจะทำให้เชื่อได้ว่า SGLT2 inhibitors สามารถช่วยในการทำให้เกิดผลลัพธ์ที่ดีในระยะยาวในผู้ป่วยที่มีภาวะไตวายเฉียบพลัน
Article Details

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
บทความนี้ตีพิมพ์ภายไต้การอนุญาต CC BY-NC-ND 4.0 ซึ่งอนุญาตให้สามารถใช้บทความนี้พื่อวัตถุประสงค์ใดๆ ก็ตามที่ไม่ใช่เชิงพาณิชย์ โดยต้องมีการอ้างถึงที่มาของบทความอย่างครบถ้วน ใครก็ตามสามารถคัดลอกและแจกจ่ายทุกส่วนของบทความนี้โดยไม่ต้องขออนุญาตจากผู้ประพันธ์หรือสมาคมโรคไตแห่งประเทศไทย
เอกสารอ้างอิง
Carlos AC, Eva R, Sheila B, Adriana S, Carla B, Clara B, et al. Short- and long-term outcomes after non-severe acute kidney injury. Clin Exp Nephrol. 2018;22(1):61-7.
Gayat E, Hollinger A, Cariou A. Deye N, Vieillard-Baron A, Jaber S, et al. Impact of angiotensin-converting enzyme inhibitors or receptor blockers in post-ICU discharge outcome in patients with acute kidney injury. Intensive Care Med. 2018;44(5):598-605.
Brar S, Ye F, James MT, Hemmelgarn B, Klarenbach S, Pannu N. Association of angiotensin-converting enzyme inhibitors or receptor blocker use with outcomes after acute kidney injury. JAMA Intern Med. 2018;178(12):1681-90.
Harel Z, Wald R, Bargman JM, Mamdani M, Etchells E, Garg AX, et al. Nephrologist follow-up improves all-cause mortality of severe acute kidney injury survivors. Kidney Int. 2013;83(5):901-8.
Thanapongsatorn P, Chaikomon K, Lumlertgul N, Yimsangyad K, Leewongwarasingh, Kulvichit W, et al. Comprehensive versus standard care in post-severe acute kidney injury survivors, a randomized controlled trial. Crit Care. 2021;25(1):322.
Kashani K, Rosner MH, Haase M, Lewington AJP, O’Donoghue DJ, Wilson FP, et al. Quality Improvement Goals for Acute Kidney Injury. Clin J Am Soc Nephrol. 2019;14(6):941-53.
Cowie MR, Fisher M. SGLT2 inhibitors: mechanisms of cardiovascular benefit beyond glycemic control. Nat Rev Cardiol. 2020;17(12):761-72.
Tahrani AA, Barnett AH, Bailey CJ. SGLT inhibitors in management of diabetes. Lancet Diabetes Endocrinol. 2013;1(2):140-51.
Griffin M, Rao VS, Ivey-Miranda J, Fleming J, Mahoney D, Maulion C, et al. Empagliflozin in heart failure: diuretic and cardiorenal effects. Circulation. 2020;142(11):1028-39.
Hallow KM, Helmlinger G, Greasley PJ, McMurray JJV, Boulton DW. Why do SGLT2 inhibitors reduce heart failure hospitalization? A differential volume regulation hypothesis. Diabetes Obes Metab. 2018;20(3):479-87.
Hiromi K, Jun S, Kazuki T, Tomoko O, Yu T, Hikaru T, et al. Effects of SGLT2 Inhibition on eGFR and Glomerular and Tubular Damage Markers in Japanese Patients with Type 2 Diabetes. J Endocrinol Metab. 2018;8(5):106-12
Foresto-Neto O, Albino AH, Arias SCA, Faustino VD, Zambom FFF, Cenedeze MA, et al. NF-κB system is chronically activated and promotes glomerular injury in experimental type 1 diabetic kidney disease. Front Physiol. 2020;11:84.
Bessho R, Takiyama Y, Takiyama T, Kitsunai H, Takeda Y, Sakagami H, et al. Hypoxia-inducible factor-1α is the therapeutic target of the SGLT2 inhibitors for diabetic nephropathy. Sci Rep. 2019;9(1):14754.
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, Cardiovascular Outcomes and Mortality in Type 2 diabetes. N Engl J Med. 2015;373(22):2117-28.
Swedberg K, Young JB, Anand IS, Cheng S, Desai AS, Diaz R, et al. Treatment of anemia with darbepoetin alfa in systolic heart failure. N Engl J Med. 2013;368(13):1210-9.
McMurray JJV, Solomon SD, Inzucchi SE, Kober L, Kosiborod MN, Martinez FA, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995-2008.
Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295–306
Cooper S, Teoh H, Campeau MA, Verma S, Leask RL. Empagliflozin restores the integrity of the endothelial glycocalyx in vitro. Mol Cell Biochem. 2019;459(1-2):121-30.
Herat LY, Magno AL, Rudnicka C, Hricova J, Carnagarin R, Ward NC et al. SGLT2 inhibitor–induced Sympathoinhibition a novel mechanism for cardiorenal protection. JACC Basic Transl Sci. 2020;5(2):169-79.
Zaccardi F, Webb DR, Htike ZZ, Youssef D, Khunti K, Davies MJ. Efficacy and safety of sodium-glucose cotransporter-2 inhibitors in type 2 diabetes mellitus: systematic review and network meta-analysis. Diabetes Obes Metab. 2016;18(8):783-94.
Chilton R, Tikkanen L, Hehnke U, Woerle HJ, Johansen OE. Impact of empagliflozin on blood pressure in dipper and non-dipper patients with type 2 diabetes mellitus and hypertension. Diabetes Obes Metab. 2017;19(11):1620-4.
Matthews V, Elliot R, Rudnicka C, Hricova J, Herat L, Schlaich M. Role of the sympathetic nervous systemin regulation of the sodium glucose co-transporter 2. J Hypertens. 2017;35(10):2059-68.
Baartscheer A, Schumacher CA, Wust RCI, Fioloet JW, Steinen GJM, Coronel R, et al. Empagliflozin decreases myocardial cytoplasmic Na+ through inhibition of the cardiac Na+/H+ exchanger in rats and rabbits. Diabetologia. 2017;60(3):568-73.
Uthman L, Baartscheer A, Bleijlevens B, Schumacher CA, Fiolet JWT, Koeman A, et al. Class effects of SGLT2 inhibitors in mouse cardiomyocytes and hearts: inhibition of Na+/H+ exchanger, lowering of cytosolic Na+ and vasodilation. Diabetologia. 2018;61(3):722-6.
Kolhaas M, Liu T, Knopp A, Zeller T, Ong MF, Böhm M, et al. Elevated cytosolic Na+ increase mitochondrial formation of reactive oxygen species in failing cardiac myocytes. Circulation. 2010;121(14):1606-13.
Ojima A, Matsui T, Nishino Y, Nakamura N, Yamagishi S. Empagliflozin, an inhibitor of sodium glucose cotransporter 2 exerts anti-inflammatory and antifibrotic effects on experimental diabetic nephropathy partly by suppressing AGEs-receptor axis. Horm Metab Res. 2015;47(9):686-92.
Kosiborod MN, Esterline RHM, Furtado R, Oscarsson J, Gasparyan SB, Koch GG, et al. Dapagliflozin in patients with cardiometabolic risk factors hospitalized with COVID-19 (DARE-19): a randomized double-blind, placebo-controlled, phase 3 trial. Lancet Diabetes Endocrinol. 2021;9(9):586-94.
Herrington WG, Staplin N, Wanner C, Green JB, Hauske SJ, Emberson JR, et al. Empagliflozin in patients with chronic kidney disease. N Engl J Med. 2023;388(2):117-27.
Gallagher M. Prevention with SGLT2 inhibition of acute kidney injury in intensive care (PREVENTS-AKI). (online). 2023. Source: https://clinicaltrials.gov/ct2/show/NCT05468203 (16th January 2023)
