
ภาวะกรดแล็กติกคั่งจากยาเมทฟอร์มิน
Article Sidebar
Main Article Content
บทคัดย่อ
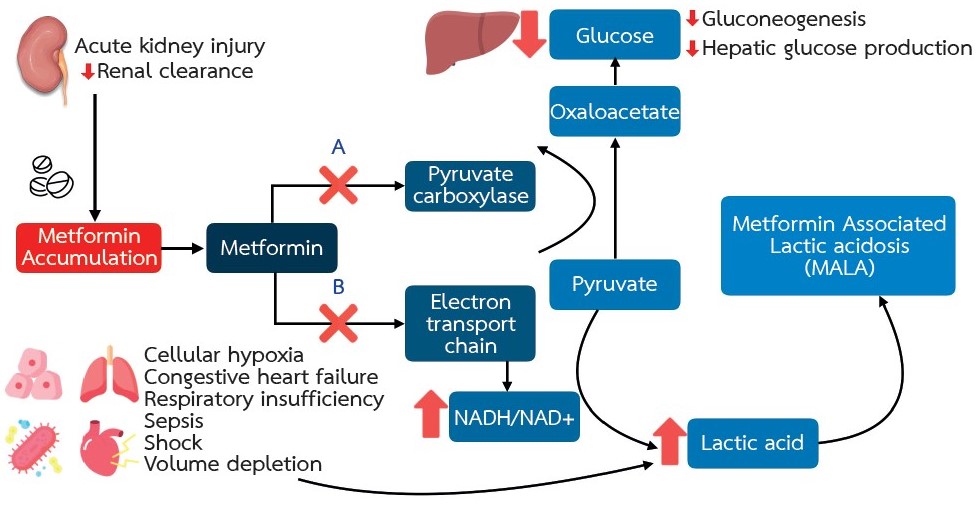
เมทฟอร์มิน (Metformin) ได้รับการแนะนำให้ใช้เป็นยาตัวแรกในการรักษาโรคเบาหวานชนิดที่ 2 จึงทำให้มีการใช้กันอย่างแพร่หลายทั่วโลก ยาเมทฟอร์มินสามารถใช้เป็นยาเบาหวานเพียงชนิดเดียว หรือใช้ร่วมกับยาเบาหวานชนิดอื่นๆ จากการศึกษาพบว่า การใช้ยาเมทฟอร์มินสามารถช่วยลดความเสี่ยงต่อการเสียชีวิตจากโรคหัวใจและหลอดเลือดอาการทางระบบทางเดินอาหารเป็นอาการไม่พึงประสงค์ที่พบได้บ่อยที่สุด ภาวะกรดแล็กติกคั่งจากยาเมทฟอร์มิน (Metformin-Associated Lactic Acidosis, MALA) เป็นอาการไม่พึงประสงค์ที่พบได้ไม่บ่อย แต่บางครั้งอาจมีอันตรายถึงแก่ชีวิต สาเหตุเกิดจากการคั่งของยาเมทฟอร์มินและกรดแล็กติกในร่างกาย เนื่องจากความสามารถในการขับยาออกจากร่างกายทางไตลดลง ผู้ป่วยจำเป็นต้องได้รับการวินิจฉัยและดูแลรักษาอย่างเร่งด่วน ซึ่งการดูแลรักษานั้นประกอบไปด้วย การติดตามอาการอย่างใกล้ชิด การรักษาภาวะสมดุลกรด-ด่างและเกลือแร่ การรักษาโรคร่วมอื่นๆ และการเร่งขจัดยาเมทฟอร์มินออกจากร่างกาย ซึ่งในกรณีที่รุนแรงอาจจำเป็นต้องอาศัยการฟอกเลือดด้วยเครื่องไตเทียม การป้องกันสามารถทำได้โดยพิจารณาใช้ยาด้วยความระมัดระวังในผู้ป่วยกลุ่มเสี่ยง และปรับขนาดยาลดลงตามระดับการทำงานของไต นอกจากนี้ ยังต้องให้คำแนะนำเพื่อเฝ้าระวังอาการของภาวะกรดแล็กติกคั่ง โดยให้หยุดยาทันทีเมื่อมีอาการดังกล่าว และเข้ารับการรักษาในโรงพยาบาลโดยเร็วที่สุด
Article Details

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
บทความนี้ตีพิมพ์ภายไต้การอนุญาต CC BY-NC-ND 4.0 ซึ่งอนุญาตให้สามารถใช้บทความนี้พื่อวัตถุประสงค์ใดๆ ก็ตามที่ไม่ใช่เชิงพาณิชย์ โดยต้องมีการอ้างถึงที่มาของบทความอย่างครบถ้วน ใครก็ตามสามารถคัดลอกและแจกจ่ายทุกส่วนของบทความนี้โดยไม่ต้องขออนุญาตจากผู้ประพันธ์หรือสมาคมโรคไตแห่งประเทศไทย
เอกสารอ้างอิง
Hadden DR. Goat's rue - French lilac - Italian fitch - Spanish sainfoin: gallega officinalis and metformin: the Edinburgh connection. J R Coll Physicians Edinb. 2005;35(3):258-60.
ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S140-S57.
Lv Z, Guo Y. Metformin and Its Benefits for Various Diseases. Front Endocrinol (Lausanne). 2020;11:191.
Foretz M, Guigas B, Bertrand L, Pollak M, Viollet B. Metformin: from mechanisms of action to therapies. Cell Metab. 2014;20(6):953-66.
Jackson RA, Hawa MI, Jaspan JB, Sim BM, Disilvio L, Featherbe D, et al. Mechanism of metformin action in non-insulin-dependent diabetes. Diabetes. 1987;36(5):632-40.
Bailey CJ, Wilcock C, Scarpello JH. Metformin and the intestine. Diabetologia. 2008;51(8):1552-3.
Bailey CJ, Turner RC. Metformin. N Engl J Med. 1996;334(9):574-9.
Graham GG, Punt J, Arora M, Day RO, Doogue MP, Duong JK, et al. Clinical pharmacokinetics of metformin. Clin Pharmacokinet. 2011;50(2):81-98.
Bonnet F, Scheen A. Understanding and overcoming metformin gastrointestinal intolerance. Diabetes Obes Metab. 2017;19(4):473-81.
Blumenberg A, Benabbas R, Sinert R, Jeng A, Wiener SW. Do Patients Die with or from Metformin-Associated Lactic Acidosis (MALA)? Systematic Review and Meta-analysis of pH and Lactate as Predictors of Mortality in MALA. J Med Toxicol. 2020;16(2):222-9.
Thammavaranucupt K, Phonyangnok B, Parapiboon W, Wongluechai L, Pichitporn W, Sumrittivanicha J, et al. Metformin-associated lactic acidosis and factors associated with 30-day mortality. PLoS One. 2022;17(8):e0273678.
Richy FF, Sabido-Espin M, Guedes S, Corvino FA, Gottwald-Hostalek U. Incidence of lactic acidosis in patients with type 2 diabetes with and without renal impairment treated with metformin: a retrospective cohort study. Diabetes Care. 2014;37(8):2291-5.
Rena G, Hardie DG, Pearson ER. The mechanisms of action of metformin. Diabetologia. 2017;60(9):1577-85.
Pham AQ, Xu LH, Moe OW. Drug-Induced Metabolic Acidosis. F1000Res. 2015;4.
Hunter RW, Hughey CC, Lantier L, Sundelin EI, Peggie M, Zeqiraj E, et al. Metformin reduces liver glucose production by inhibition of fructose-1-6-bisphosphatase. Nat Med. 2018;24(9):1395-406.
Hur KY, Lee MS. New mechanisms of metformin action: Focusing on mitochondria and the gut. J Diabetes Investig. 2015;6(6):600-9.
DeFronzo R, Fleming GA, Chen K, Bicsak TA. Metformin-associated lactic acidosis: Current perspectives on causes and risk. Metabolism. 2016;65(2):20-9.
Asif S, Bennett J, Marakkath B. Metformin-associated Lactic Acidosis: An Unexpected Scenario. Cureus. 2019;11(4):e4397.
Ashraf S, Upreti P, Karki S, Khan M, Nasr R. Metformin-Associated Lactic Acidosis: A Case Report and Review. Cureus. 2022;14(4):e24220.
Schadle P, Tschritter O, Kellerer M. Metformin Associated Lactic Acidosis in Clinical Practice - A Case Series. Exp Clin Endocrinol Diabetes. 2021;129(11):842-7.
Gan SC, Barr J, Arieff AI, Pearl RG. Biguanide-associated lactic acidosis. Case report and review of the literature. Arch Intern Med. 1992;152(11):2333-6.
Almirall J, Briculle M, Gonzalez-Clemente JM. Metformin-associated lactic acidosis in type 2 diabetes mellitus: incidence and presentation in common clinical practice. Nephrol Dial Transplant. 2008;23(7):2436-8.
Lalau JD, Lemaire-Hurtel AS, Lacroix C. Establishment of a database of metformin plasma concentrations and erythrocyte levels in normal and emergency situations. Clin Drug Investig. 2011;31(6):435-8.
Kraut JA, Madias NE. Metabolic acidosis: pathophysiology, diagnosis and management. Nat Rev Nephrol. 2010;6(5):274-85.
Lalau JD, Race JM. Lactic acidosis in metformin-treated patients. Prognostic value of arterial lactate levels and plasma metformin concentrations. Drug Saf. 1999;20(4):377-84.
Teale KF, Devine A, Stewart H, Harper NJ. The management of metformin overdose. Anaesthesia. 1998;53(7):698-701.
Feeney-Stewart F. The sodium bicarbonate controversy. Dimens Crit Care Nurs. 1990;9(1):22-8.
Cuhaci B, Lee J, Ahmed Z. Sodium bicarbonate controversy in lactic acidosis. Chest. 2000;118(3):882-4.
Rosival V. Evaluating sodium bicarbonate controversy. Chest. 2001;119(5):1622-3.
Calello DP, Liu KD, Wiegand TJ, Roberts DM, Lavergne V, Gosselin S, et al. Extracorporeal Treatment for Metformin Poisoning: Systematic Review and Recommendations From the Extracorporeal Treatments in Poisoning Workgroup. Crit Care Med. 2015;43(8):1716-30.
Harding SA, Biary R, Hoffman RS, Su MK, Howland MA. A Pharmacokinetic Analysis of Hemodialysis for Metformin-Associated Lactic Acidosis. J Med Toxicol. 2021;17(1):70-4.
Correia MS, Horowitz BZ. Continuous extracorporeal clearance in metformin-associated lactic acidosis and metformin-induced lactic acidosis: a systematic review. Clin Toxicol (Phila). 2022;60(11):1266-76.
Deepak V, Neel S, Lohana AC, Tanase A. Metformin-associated Lactic Acidosis Successfully Treated with Continuous Renal Replacement Therapy. Cureus. 2019;11(8):e5330.
Regolisti G, Antoniotti R, Fani F, Greco P, Fiaccadori E. Treatment of Metformin Intoxication Complicated by Lactic Acidosis and Acute Kidney Injury: The Role of Prolonged Intermittent Hemodialysis. Am J Kidney Dis. 2017;70(2):290-6.
Navaneethan SD, Zoungas S, Caramori ML, Chan JCN, Heerspink HJL, Hurst C, et al. Diabetes Management in Chronic Kidney Disease: Synopsis of the KDIGO 2022 Clinical Practice Guideline Update. Ann Intern Med. 2023;176(3):381-7.
Hanna RM, Rhee CM, Kalantar-Zadeh K. Metformin in chronic kidney disease: a strong dose of caution. Kidney Int. 2020;98(5):1101-5.
Jones GC, Macklin JP, Alexander WD. Contraindications to the use of metformin. BMJ. 2003;326(7379):4-5.
Landewe-Cleuren S, van Zwam WH, de Bruin TW, de Haan M. [Prevention of lactic acidosis due to metformin intoxication in contrast media nephropathy]. Ned Tijdschr Geneeskd. 2000;144(40):1903-5.
