
Serum Galectin-3 as a diagnostic and discriminatory biomarker for chronic kidney disease: A case-control study
Article Sidebar
Main Article Content
Abstract
Background: Diabetic kidney disease (DKD) is the leading cause of end-stage renal disease worldwide. Conventional markers, such as serum creatinine, estimated glomerular filtration rate, and albuminuria, have limited sensitivity for distinguishing among etiologies of advanced chronic kidney disease (CKD) and become abnormal only after substantial nephron loss. Galectin-3 (GAL-3), a beta-galactoside-binding lectin implicated in renal inflammation and fibrosis, has emerged as a candidate biomarker; however, its diagnostic accuracy in distinguishing DKD from non-diabetic CKD in advanced CKD populations remains unclear.
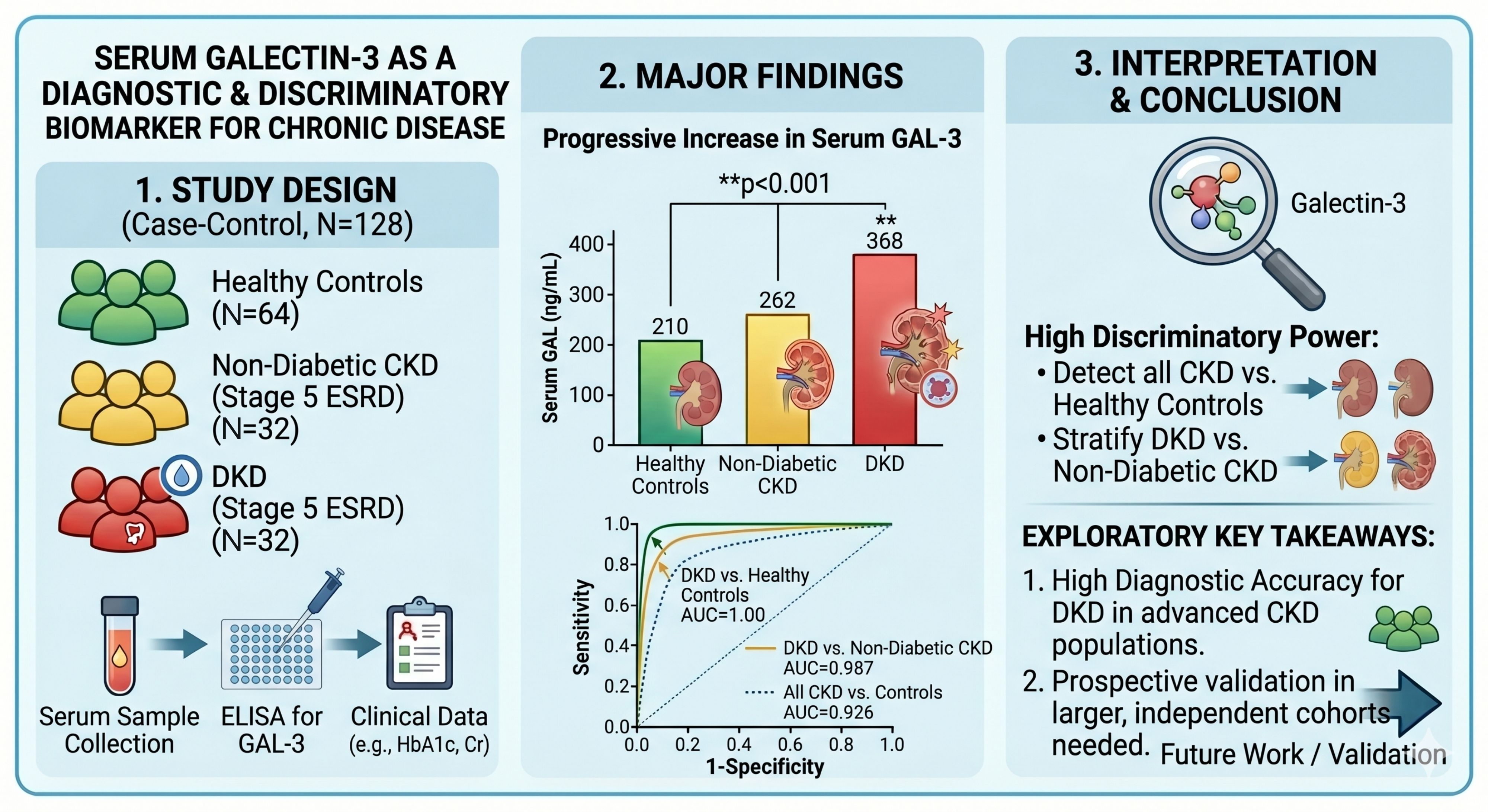
Objective: To quantify serum GAL-3 concentrations in patients with DKD, non-diabetic CKD, and healthy controls, and to evaluate its diagnostic performance in discriminating between these groups in an advanced CKD population.
Materials and methods: A case-control study that enrolled 128 participants: 32 patients with DKD (all with type 2 diabetes mellitus), 32 with non-diabetic CKD (both groups on regular hemodialysis classified as CKD stage 5/end-stage renal disease [ESRD]), and 64 healthy controls. Serum GAL-3 levels were measured using an enzyme-linked immunosorbent assay (ELISA). Fasting blood glucose, glycated hemoglobin (HbA1c), renal function tests, and serum albumin levels were assessed using an automated analyzer.
Results: Serum GAL-3 concentrations increased progressively from controls (210.04±34.65 ng/mL) to non-diabetic CKD (262.21±3.19 ng/mL) and then to DKD (368.50±67.10 ng/mL, p<0.001). Receiver operating characteristic (ROC) analysis demonstrated very high discrimination in this cohort between DKD and healthy controls area under the curve (AUC=1.00, 95% CI: 0.963-1.000, sensitivity, 100%, specificity, 100%; cutoff, ≥275.77 ng/mL), excellent differentiation of DKD from non-diabetic CKD (AUC=0.987, 95% CI: 0.905-0.999, sensitivity, 84.37%, specificity, 100%), and strong discrimination of all CKD patients from controls (AUC=0.926, 95% CI: 0.866-0.965; sensitivity, 98.44%, specificity, 73.44%). These cutoff values were derived from the same dataset and should be considered exploratory.
Conclusion: Serum GAL-3 demonstrated very high diagnostic accuracy in identifying and stratifying DKD within this cohort of end-stage renal disease patients on hemodialysis. These exploratory findings suggest that GAL-3 may have potential as a discriminatory biomarker in advanced CKD populations; however, prospective validation in larger, independent cohorts including patients with early-stage CKD is warranted before clinical integration can be recommended.
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Personal views expressed by the contributors in their articles are not necessarily those of the Journal of Associated Medical Sciences, Faculty of Associated Medical Sciences, Chiang Mai University.
References
Jager KJ, Kovesdy C, Langham R, Rosenberg M, Jha V, Zoccali C. A single number for advocacy and communication-worldwide more than 850 million individuals have kidney diseases. Nephrol Dial Transplant 2019; 34: 1803-5. doi: 10.1093/ndt/gfz174.
Alicic RZ, Rooney MT, Tuttle KR. Diabetic kidney disease: challenges, progress, and possibilities. Clin J Am Soc Nephrol 2017; 12: 2032-45. doi: 10.2215/CJN.11491116.
Sinha SK, Nicholas SB. Pathomechanisms of diabetic kidney disease. J Clin Med 2023; 12: 7349. doi: 10.3390/jcm12237349.
Shahbazian H, Rezaii I. Diabetic kidney disease; review of the current knowledge. J Ren Inj Prev 2013; 2: 73. doi: 10.12861/jrip.2013.24.
Atlas D. International diabetes federation. IDF Diabetes Atlas, 7th Ed. Brussels, Belgium Int Diabetes Fed 2015; 33.
Liu Z, Liu J, Wang W, An X, Luo L, Yu D, et al. Epigenetic modification in diabetic kidney disease. Front Endocrinol (Lausanne) 2023; 14: 1133970. doi: 10.3389/fendo.2023.1133970.
Lin C-H, Chang Y-C, Chuang L-M. Early detection of diabetic kidney disease: Present limitations and 176 Nasser AH and Sarhat ER. Journal of Associated Medical Sciences 2026; 59(3): 168-176 future perspectives. World J Diabetes 2016; 7: 290. doi: 10.4239/wjd.v7.i14.290.
Dopierała M, Nitz N, Król O, Wasicka-Przewoźna K, Schwermer K, Pawlaczyk K. New and emerging biomarkers in chronic kidney disease. Biomedicines 2025; 13: 1423. doi: 10.3390/biomedicines13061423.
Hussain S, Jamali MC, Habib A, Hussain MS, Akhtar M, Najmi AK. Diabetic kidney disease: An overview of prevalence, risk factors, and biomarkers. Clin Epidemiol Glob Heal 2021; 9: 2-6. doi: 10.1016/j.cegh.2020.05.016.
Syn G, Lee YQ, Lim ZY, Chan GC. Galectin-3: action and clinical utility in chronic kidney disease. Int Urol Nephrol 2024; 56: 3535-43. doi: 10.1007/s11255-024-04107-4.
Bellos I, Marinaki S, Lagiou P, Benetou V. Association of serum galectin-3 levels with mortality and cardiovascular disease outcomes in hemodialysis patients: a systematic review and dose-response meta-analysis. Int Urol Nephrol 2024; 56: 2755-67. doi: 10.1007/s11255-024-04026-4.
Ameer Mahdi N, Choobineh H, Hashim Abdulsalam A, Majidi Z, Dashti N. Elevated serum levels of Galectin-3 and Kidney Injury Molecule-1 as potential biomarkers for early detection and staging of chronic kidney disease in Iraqi population. Reports Biochem Mol Biol 2025; 14: 95-101. doi: 10.61882/rbmb.14.1.95.
Wang F, Zhou L, Eliaz A, Hu C, Qiang X, Ke L, et al. The potential roles of galectin-3 in AKI and CKD. Front Physiol 2023; 14: 1090724. doi: 10.3389/fphys.2023.1090724.
Chen Y, Jiang Q, Xing X, Xu L, Zhao Q, Zhang Q, et al. Macrophage derived Galectin-3 promotes renal fibrosis and diabetic kidney disease by enhancing TGFβ1 signaling. Adv Sci (Weinheim, Baden-Wurttemberg, Ger 2025; 12: e04032. doi: 10.1002/advs.202504032.
Karimi F, Moazamfard M, Taghvaeefar R, Sohrabipour S, Dehghani A, Azizi R, et al. Early detection of diabetic nephropathy based on urinary and serum biomarkers: An updated systematic review. Adv Biomed Res 2024; 13: 104. doi: 10.4103/abr.abr_461_23.
Bellos I, Marinaki S, Lagiou P, Benetou V. Galectin-3 in chronic kidney disease. Clin Chim Acta 2024; 559: 119727. doi: 10.1016/j.cca.2024.119727.
Hodeib H, Hagras MM, Abdelhai D, Watany MM, Selim A, Tawfik MA, et al. Galectin-3 as a prognostic biomarker for diabetic nephropathy. Diabetes, Metab Syndr Obes Targets Ther 2019: 325-31. doi: 10.2147/DMSO.S194410.
Buliga-Finis ON, Ouatu A, Tanase DM, Badescu MC, Dima N, Gosav EM, et al. The role of Galectin-3 as a biomarker in the cardio-renal-metabolic Pathology Axis. J Clin Med 2025; 14. doi: 10.3390/jcm14176071.
Tan KCB, Cheung C-L, Lee ACH, Lam JKY, Wong Y, Shiu SWM. Galectin-3 is independently associated with progression of nephropathy in type 2 diabetes mellitus. Diabetologia 2018; 61: 1212–9. doi: 10.1007/s00125-018-4552-z.
Guo Y, Li L, Hu S. Circulating Galectin-3 levels and diabetic nephropathy: a systematic review and meta-analysis. BMC Nephrol 2023; 24: 163. doi: 10.1186/s12882-023-03226-x.
