
The re-emerging shadow: A systematic review of scrub typhus in India
Article Sidebar
Main Article Content
Abstract
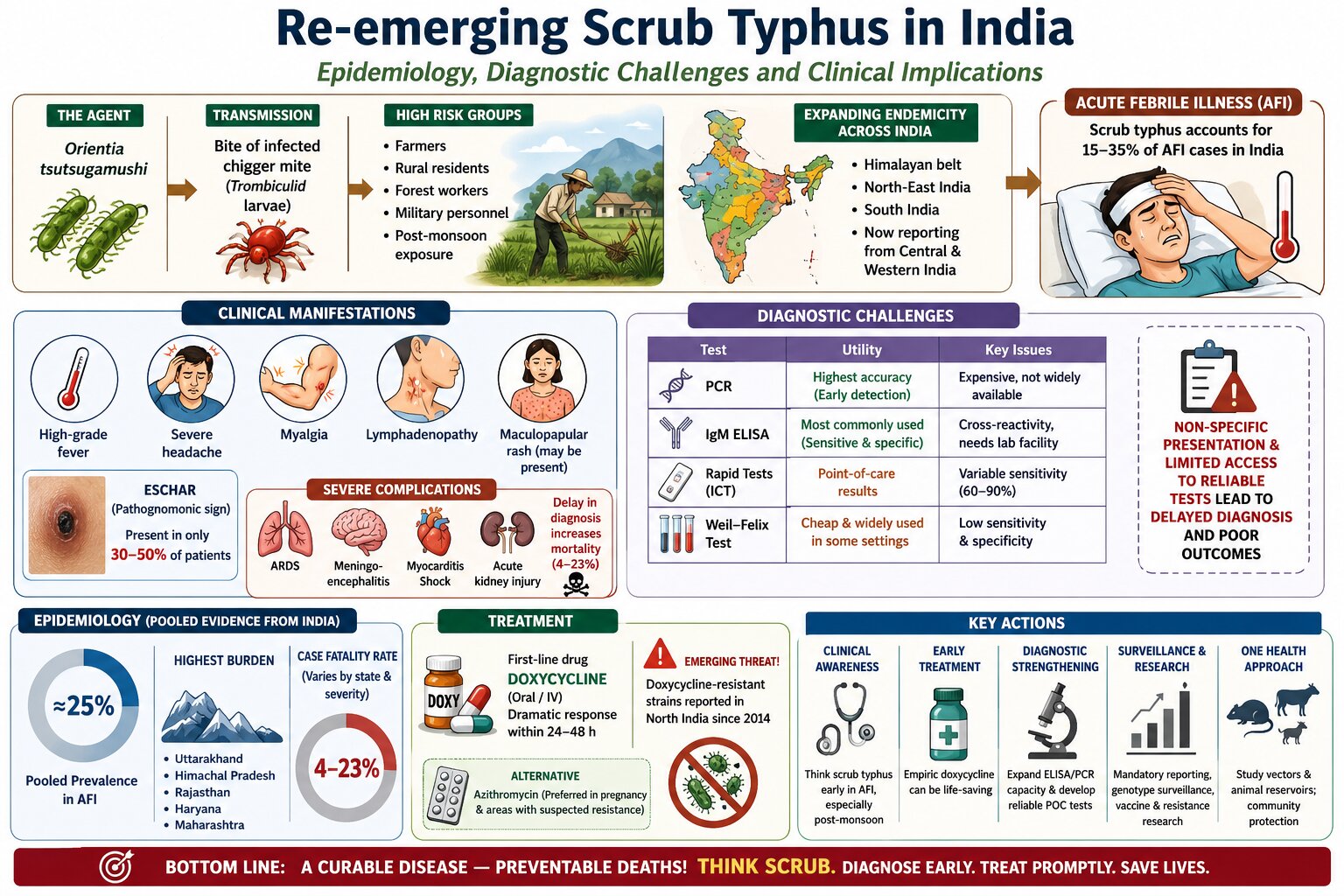
Background: Scrub typhus, caused by Orientia tsutsugamushi and transmitted by larval trombiculid mites, has re-emerged as an important cause of acute febrile illness (AFI) in India. The disease is frequently underdiagnosed because of its non-specific clinical presentation, variable occurrence of eschar, and limited availability of reliable diagnostic facilities. Delayed diagnosis and treatment may result in severe complications and significant mortality.
Objectives: To systematically review the available literature on scrub typhus in India and to assess its epidemiology, pooled prevalence among patients with acute febrile illness, case fatality rate (CFR), clinical manifestations, diagnostic challenges, treatment outcomes, and emerging public health concerns.
Materials and methods: A systematic review of the published literature from 2013 to 2023 was conducted in accordance with the PRISMA 2020 guidelines. Electronic databases, including PubMed, Google Scholar, and Indian biomedical journals, were searched using predefined keywords related to scrub typhus and acute febrile illness. Two independent reviewers screened studies, extracted data, and assessed eligibility. Information regarding epidemiology, diagnostic methods, clinical features, prevalence, CFR, and treatment outcomes was synthesized. Heterogeneity among studies was assessed using the I² statistic, and sensitivity analysis was performed by excluding studies utilizing the Weil–Felix test.
Results: Scrub typhus has emerged as a major contributor to acute febrile illness across India, particularly in the Himalayan region, northeastern states, and southern India, with increasing reports from western and central regions. Pooled analyses indicate that approximately one-fourth of patients presenting with acute febrile illness are positive for scrub typhus. State-specific prevalence ranged from 15% to over 50%, while pooled CFR varied from <5% to over 20% depending on disease severity and healthcare setting. High heterogeneity was observed across studies (I² range: 32-71%), largely attributable to differences in diagnostic methods and study populations. Sensitivity analysis showed an increase in pooled prevalence from approximately 24% to 29% after excluding Weil-Felix-based studies, suggesting that less sensitive diagnostic methods underestimate the disease burden. Common clinical manifestations included high-grade fever, headache, myalgia, lymphadenopathy, and elevated live enzymes, whereas eschar was present in only 30-50% of patients. Severe complications included acute respiratory distress syndrome, meningoencephalitis, myocarditis, acute kidney injury, and shock. Doxycycline remained the cornerstone of therapy, although emerging reports of reduced treatment response have raised concerns regarding antimicrobial resistance.
Conclusion: Scrub typhus is a significant and growing public health challenge in India, accounting for a substantial proportion of acute febrile illness and preventable mortality. Early clinical suspicion, prompt initiation of appropriate antimicrobial therapy, improved access to reliable diagnostics, strengthened surveillance systems, and continued monitoring of circulating genotypes are essential for reducing disease burden and improving patient outcomes. Greater integration of clinical, laboratory, epidemiological, and One Health approaches is required to address the re-emergence of scrub typhus in India.
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Personal views expressed by the contributors in their articles are not necessarily those of the Journal of Associated Medical Sciences, Faculty of Associated Medical Sciences, Chiang Mai University.
References
Sharma N, Biswal M, Kumar A, Zaman K, Jain S, Bhalla A. Scrub typhus in a tertiary care hospital in North India. Am J Trop Med Hyg. 2016; 95(2): 447-51. doi: 10.4269/ajtmh.16-0086.
Stephen S, Kandhakumari G, Pradeep J, Vinithra SM, Siva PK, Hanifah M, et al. Scrub typhus in South India: a re-emerging infectious disease. Jpn J Infect Dis. 2013; 66(6): 552-4. doi: 10.7883/yoken.66.552.
Rathi N, Rathi A. Rickettsial infections: Indian perspective. Indian Pediatr. 2010; 47(2): 157-64. doi: 10.1007/s13312-010-0024-3.
Varghese GM, Janardhanan J, Trowbridge P, Peter JV, Prakash JAJ, Sathyendra S, et al. Scrub typhus in South India: clinical and laboratory manifestations, genetic variability, and outcome. Int J Infect Dis. 2013; 17(11): e981-e988. doi: 10.1016/j.ijid.2013.05.017.
Rajapakse S, Rodrigo C, Fernando D. Drug treatment of scrub typhus: a systematic review and meta-analysis of controlled clinical trials. Trans R Soc Trop Med Hyg. 2012; 106(6): 336-44. doi: 10.1016/j.trstmh.2012.01.004.
Mittal M, Thangaraj JWV, Rose W, Velayudhan A, Kumar S, Kumar MS, et al. Scrub typhus as a cause of acute encephalitis syndrome, Gorakhpur, Uttar Pradesh, India. Emerg Infect Dis. 2017; 23(8): 1414-6. doi: 10.3201/eid2308.170025.
Abhilash KPP, Jeevan JA, Mitra S, Paul N, Murugan TP, Rupa V, et al. Acute undifferentiated febrile illness in patients presenting to a tertiary care hospital in South India: clinical spectrum and outcome. J Glob Infect Dis. 2016; 8(4): 147-54. doi: 10.4103/0974-777X.192964.
Peter JV, Sudarsan TI, Prakash JAJ, Varghese GM. Severe scrub typhus infection: clinical features, diagnostic challenges and management. World J Crit Care Med. 2015; 4(3): 244-50. doi: 10.5492/wjccm.v4.i3.244.
Kumar S, Kumar M, Aggarwal B, Kumari R. Scrub typhus in children: Clinical profile and complications at a Tertiary Care Teaching Hospital in Uttarakhand. Indian J Child Health. 2017; 4(2): 188-92. doi: 10.32677/IJCH.2017.v04.i02.018.
Sharma PK, Ramakrishnan R, Hutin YJF, Barui AK, Manickam P, Kakkar M, et al. Scrub typhus in Darjeeling, India: opportunities for simple, practical prevention measures. Trans R Soc Trop Med Hyg. 2009; 103(11): 1153-8. doi: 10.1016/j.trstmh.2009.02.006.
Blacksell SD, Bryant NJ, Paris DH, Doust JA, Sakoda Y, Day NPJ. Scrub typhus serologic testing with the indirect immunofluorescence assay as a diagnostic gold standard: a lack of consensus leads to a lot of confusion. Clin Infect Dis. 2007; 44(3): 391-401. doi: 10.1086/510585.
Koraluru M, Bairy I, Varma M, Vidyasagar S. Diagnostic validation of selected serological tests for detecting scrub typhus. Microbiol Immunol. 2015; 59(7): 371-4. doi:10.1111/1348-0421.12265.
Gupta N, Kumar TP, Boodman C, Fontaine K, Bottieau E. Frequency and distribution of eschar in patients with scrub typhus in India: systematic review of literature and meta-analysis. Infez Med. 2024; 32(3): 312-22.
Devasagayam E, Dayanand D, Kundu D, Kamath MS, Kirubakaran R, Varghese GM. The burden of scrub typhus in India: a systematic review. PLoS Negl Trop Dis. 2021; 15(7): e0009619. doi: 10.1371/journal.pntd.0009619.
Sondhiya G, Manjunathachar HV, Singh P, Kumar R. Unveiling the burden of scrub typhus in acute febrile illness cases across India: A systematic review & meta-analysis. Indian J Med Res. 2024; 159(6): 601-18. doi: 10.25259/ijmr_1442_23.
Nallan K, Kalidoss BC, Jacob ES, Kumar S, Elchuri S, Khurana S, et al. A novel genotype of Orientia tsutsugamushiin human cases of scrub typhus from Southeastern India. Microorganisms. 2025; 13(2): 333. doi: 10.3390/microorganisms13020333.
Govindarajan R, Sankar SG, Kumar MS, Krishnamoorthi R, Kumar AN, Lalitha K, et al. Molecular detection of Orientia tsutsugamushi in ectoparasites & their small mammal hosts captured from scrub typhus endemic areas in Madurai district, India. Indian J Med Res. 2024; 159(2): 180-92. doi: 10.4103/ijmr.ijmr_3530_21.
