
Dual-scale evaluation of pain after hypofractionated post-mastectomy radiotherapy
Article Sidebar
Main Article Content
Abstract
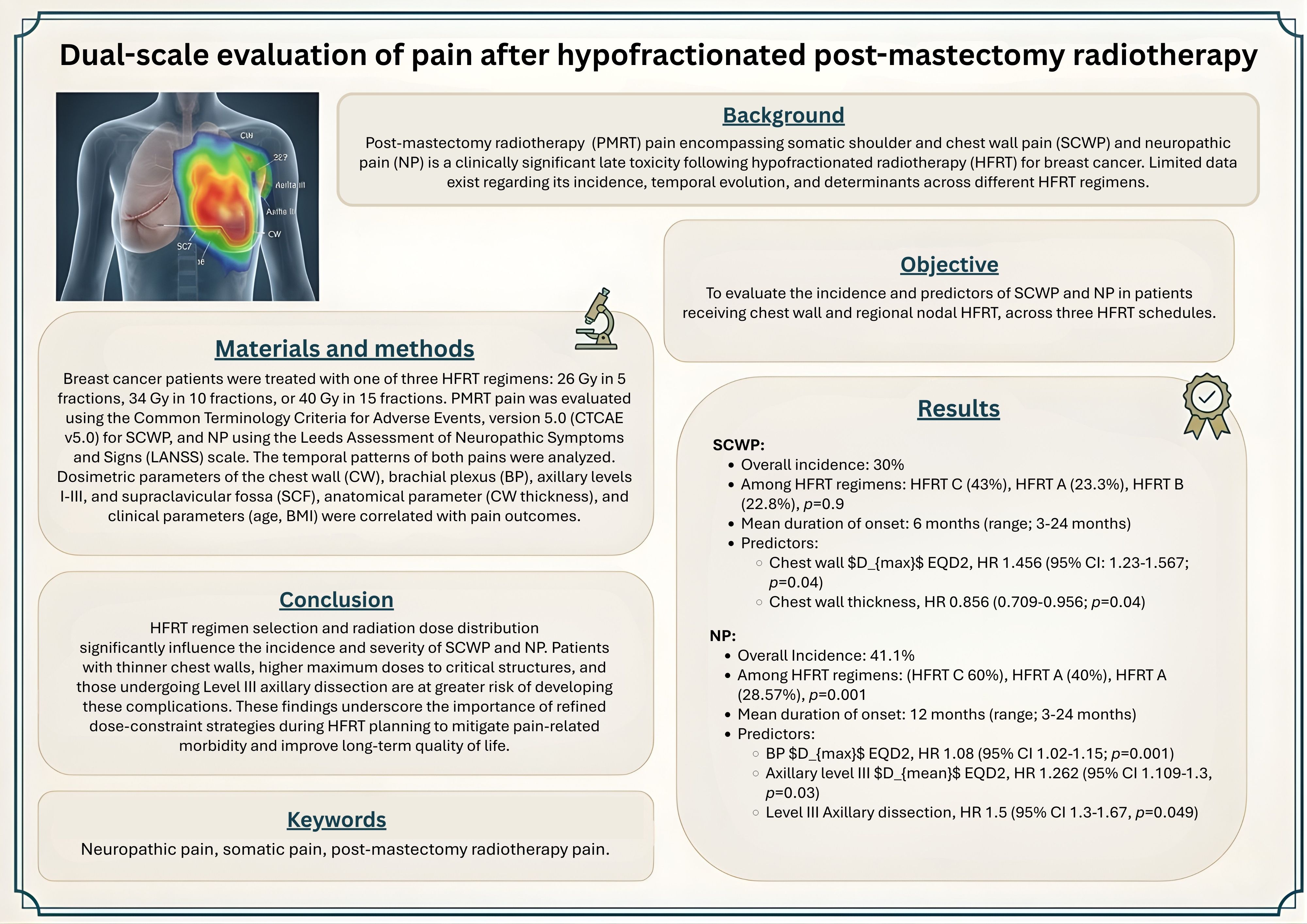
Background: Post-mastectomy radiotherapy (PMRT) pain encompassing somatic shoulder and chest wall pain (SCWP) and neuropathic pain (NP) is a clinically significant late toxicity following hypofractionated radiotherapy (HFRT) for breast cancer. Limited data exist regarding its incidence, temporal evolution, and determinants across different HFRT regimens.
Objectives: To evaluate the incidence and predictors of SCWP and NP in patients receiving chest wall and regional nodal HFRT, across three HFRT schedules.
Materials and methods: Breast cancer patients were treated with one of three HFRT regimens: 26 Gy in 5 fractions, 34 Gy in 10 fractions, or 40 Gy in 15 fractions. PMRT pain was evaluated using the Common Terminology Criteria for Adverse Events, version 5.0 (CTCAE v5.0) for SCWP, and NP using the Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) scale. The temporal patterns of both pains were analyzed. Dosimetric parameters of the chest wall (CW), brachial plexus (BP), axillary levels I-III, and supraclavicular fossa (SCF), anatomical parameter (CW thickness), and clinical parameters (age, BMI) were correlated with pain outcomes.
Results: The mean duration of SCWP was 6 months (range, 3-36 months), which was most frequently observed with HFRT-C (40%), followed by HFRT-B (22.9%) and HFRT-A (23.3%) (p=0.09). Patients with Grade≥2 SCWP had significantly thinner CW (p=0.04) and higher CW Dmax EQD2 values (p=0.04). NP occurred with a mean onset of 12 months (range, 3-24 months) and was most common in HFRT-C (60%), versus 40% in HFRT-A and 28.6% in HFRT-B (p=0.001). On multivariate analysis, Level III axillary dissection (0.049) and higher BP Dmax EQD2(p=0.001), axillary level III Dmean EQD2 (p=0.049) were found to be significant predictors of NP.
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Personal views expressed by the contributors in their articles are not necessarily those of the Journal of Associated Medical Sciences, Faculty of Associated Medical Sciences, Chiang Mai University.
References
Andersen KG, Kehlet H. Persistent pain after breast cancer treatment: a critical review of risk factors and strategies for prevention. J Pain. 201; 12(7): 725-46. doi: 10.1016/j.jpain.2010.12.005.
Smith HS, Wu SX. Persistent pain after breast cancer treatment. Ann Palliat Med. 2012; 1(3): 182-94. doi: 10.3978/j.issn.2224-5820.2012.10.13.
Bennett MI, Rayment C, Hjermstad M, Aass N, Caraceni A, Kaasa S. Prevalence and aetiology of neuropathic pain in cancer patients: A systematic review. PAIN. 2012; 153(2): 359-65. doi: 10.1016/j.pain.2011.10.028.
Voruganti IS, Donovan E, Walker-Dilks C, Swaminath A. Chest wall toxicity after stereotactic radiation in early lung cancer: a systematic review. Curr Oncol. 2020; 27(4): 179-89. doi: 10.3747/co.27.5959.
Wang L, Guyatt GH, Kennedy SA, Romerosa B, Kwon HY, Kaushal A, et al. Predictors of persistent pain after breast cancer surgery: a systematic review and meta-analysis of observational studies. CMAJ. 2016; 188(14): E352-61. doi: 10.1503/cmaj.151276.
Fijardo M, Kwan JYY, Bissey PA, Citrin DE, Yip KW, Liu FF. The clinical manifestations and molecular pathogenesis of radiation fibrosis. eBioMedicine. 2024; 103: 105089. doi: 10.1016/j.ebiom.2024.105089.
Kim JS, Spiess AM. Surgical treatment of intercostal brachial nerve pain after mastectomy and axillary dissection. Plast Reconstr Surg Glob Open. 2021; 9(11): e3935. doi: 10.1097/GsOX.0000000000003935.
Yan M, Kong W, Kerr A, Brundage M. The radiation dose tolerance of the brachial plexus: a systematic review and meta-analysis. Clin Transl Radiat Oncol. 2019; 18: 23-31. doi: 10.1016/j.ctro.2019.06.006.
Andolino DL, Forquer JA, Henderson MA, Barriger RB, Shapiro RH, Brabham JG, et al. Maximum dose to chest wall greater than 60 Gy and volume of chest wall receiving greater than 30 Gy predict risk of chest wall toxicity following stereotactic body radiation therapy (SBRT). Int J Radiat Oncol Biol Phys. 2009; 75(3): S60. doi: 10.1016/j.ijrobp.2009.07.156.
Calapai M, Esposito E, Puzzo L, Vecchio DA, Blandino R, Bova G, et al. Post-mastectomy pain: An updated overview on risk factors, predictors, and markers. Life. 2021; 11(10): 1026. doi: 10.3390/life11101026.
Sun KY, Hall WH, Mathai M, Dublin AB, Gupta V, Purdy JA, et al. Validating the RTOG-endorsed brachial plexus contouring atlas: An evaluation of reproducibility among patients treated by intensity-modulated radiotherapy for head-andneck cancer. Int J Radiat Oncol Biol Phys. 2012; 82(3): 1060-4. doi: 10.1016/j.ijrobp.2010.10.035.
Vargo JA, Beriwal S. RTOG chest wall contouring guidelines for post-mastectomy radiation therapy: is it evidence-based?. Int J Radiat Oncol Biol Phys. 2015; 93(2): 266. doi: 10.1016/j.ijrobp. 2015.03.001.
Kakati B, Nair N, Chatterjee A. Post mastectomy pain syndrome at an Indian tertiary cancer centre and its impact on quality of life. Indian J Cancer. 2023; 60(2): 275-81. doi: 10.4103/ijc.ijc_861_21.
Yadav BS, Bansal A, Kuttikat PG, Das D, Gupta A, Dahiya D. Late-term effects of hypofractionated chest wall and regional nodal radiotherapy with two-dimensional technique in patients with breast cancer. Radiat Oncol J. 2020; 38(2): 109-18. doi: 10.3857/roj.2020.00129.
Haviland JS, Bentzen SM, Bliss JM, Yarnold JR. Prolongation of overall treatment time as a cause of treatment failure in early breast cancer: An analysis of the UK START (standardisation of breast radiotherapy) trials of radiotherapy fractionation. Radiother Oncol. 2016; 121(3): 420-3. doi: 10.1016/j.radonc.2016.08.027.
Delanian S, Lefaix JL, Pradat PF. Radiation-induced neuropathy in cancer survivors. Radiother Oncol. 2012; 105(3): 273-82. doi: 10.1016/j.radonc.2012.10.012.
Kang KH, Okoye CC, Patel RB, Siva S, Biswas T, Ellis RJ, Yao M, Machtay M, Lo SS. Complications from stereotactic body radiotherapy for lung cancer. Cancers. 2015; 7(2): 98-1004. doi.org/ 10.3390/cancers7020820.
Chang, P., Wu, S. & Emos, M.R. Identification, Evaluation, and Management of Post-breast Surgery Pain Syndrome. Curr Phys Med Rehabil Rep. 2024; 12, 161-9. doi: 10.1007/s40141-024-00438-6.
Lundstedt D, Lindberg A, Gustafsson M, Chakarova R, Karlsson P. Adjuvant radiation treatment of breast cancer after mastectomy: Advanced algorithms and partial bolus improve the dose calculation accuracy in the case of thinchest-wall irradiation. Adv Radiat Oncol. 2023; 8(5): 101223. doi: 10.1016/j.adro.2023.101223.
Kim D, Kim K, Kim JS, Kang S, Park JM, Shin KH. Near-maximum rib dose is the most relevant risk factor for ipsilateral spontaneous rib fracture: a dosimetric analysis of breast cancer patients after radiotherapy. Strahlenther Onkol. 2023; 199(1): 38-47. doi: 10.1007/s00066-022-01972-9.
Kapitanova I, Biswas S, Divekar S, Kemmerer EJ, Rostock RA, Forster KM, et al. Estimating the tolerance of brachial plexus to hypofractionated stereotactic body radiotherapy: a modellingbased approach from clinical experience. Radiat Oncol. 2021; 16(1): 98. doi: 10.1186/s13014-021-01822-5.
Gałecki J, Hicer-Grzenkowicz J, Grudzień-Kowalska M, Michalska T, Załucki W. Radiationinduced brachial plexopathy and hypofractionated regimens in adjuvant irradiation of patients with breast cancer-a review. Acta Oncol. 2006; 45(3): 280-4. doi: 10.1080/02841860500371907.
Olsen NK, Pfeiffer P, Johannsen L, Schrøder H, Rose C. Radiation-induced brachial plexopathy: neurological follow-up in 161 recurrence-free breast cancer patients. Int J Radiat Oncol Biol Phys. 1993; 26(1): 43-9. doi: 10.1016/0360-3016(93)90171-Q.
Lundstedt D, Gustafsson M, Steineck G, Sundberg A, Wilderäng U, Holmberg E, et al. Radiation therapy to the plexus brachialis in breast cancer patients: Analysis of paresthesia in relation to dose and volume. Int J Radiat Oncol Biol Phys. 2015; 92(2): 277-83. doi: 10.1016/j.ijrobp.2015.01.016.
Vecht CJ, Van de Brand HJ, Wajer OJ. Post-axillary dissection pain in breast cancer due to a lesion of the intercostobrachial nerve. Pain. 1989; 38(2): 171-6. doi: 10.1016/0304-3959(89)90235-2.
Cui L, Fan P, Qiu C, Hong Y. Single institution analysis of incidence and risk factors for postmastectomy pain syndrome. Sci. Rep. 2018; 8(1): 11494. doi: 10.1038/s41598-018-29946-x.
Kaur N, Kumar R, Jain A, Saxena AK. Sensory changes and postmastectomy pain following preservation of intercostobrachial nerve in breast cancer surgery: a prospective randomized study. Indian J Surg Oncol. 2021; 12(1): 108-13. doi: 10.1007/s13193-020-01193-5.
Goyal S, Menon D, Puzhakkal N, Makuny D. Brachial plexus doses in locoregional radiotherapy for breast cancer. TRO. 2019; 3. doi: 10.21037/tro.2019.08.03.
Rudra S, Roy A, Brenneman R, Gabani P, Roach MC, Ochoa L, et al. Radiation-induced brachial plexopathy in patients with breast cancer treated with comprehensive adjuvant radiation Therapy. Adv Radiat Oncol. 2020; 6(1): 100602. doi: 10.1016/j.adro.2020.10.015.
Wu SG, Huang SJ, Zhou J, Sun JY, Guo H, Li FY, et al. Dosimetric analysis of the brachial plexus among patients with breast cancer treated with post-mastectomy radiotherapy to the ipsilateral supraclavicular area: report of 3 cases of radiationinduced brachial plexus neuropathy. Radiat Oncol. 2014; 9: 292. doi: 10.1186/s13014-014-0292-5.
