
The study of maximum electromyogram of masseter muscle before and during modified electroconvulsive therapy in psychiatric patients
Article Sidebar
Main Article Content
Abstract
Background: Electroconvulsive therapy (ECT) is generally used to treat various severe and treatment resistant psychiatric disorders. Nowadays modified ECT is used, injury to teeth and other oral structure remain a risk in ECT despite the use of muscle relaxants due to the electrodes are placed on the temporal, quite close to the masseter muscle. The use of a bite guard is essential to prevent dental and soft tissue injuries; however, limited evidence exists regarding electromyogram (EMG) of the masseter muscle before and during modified ECT.
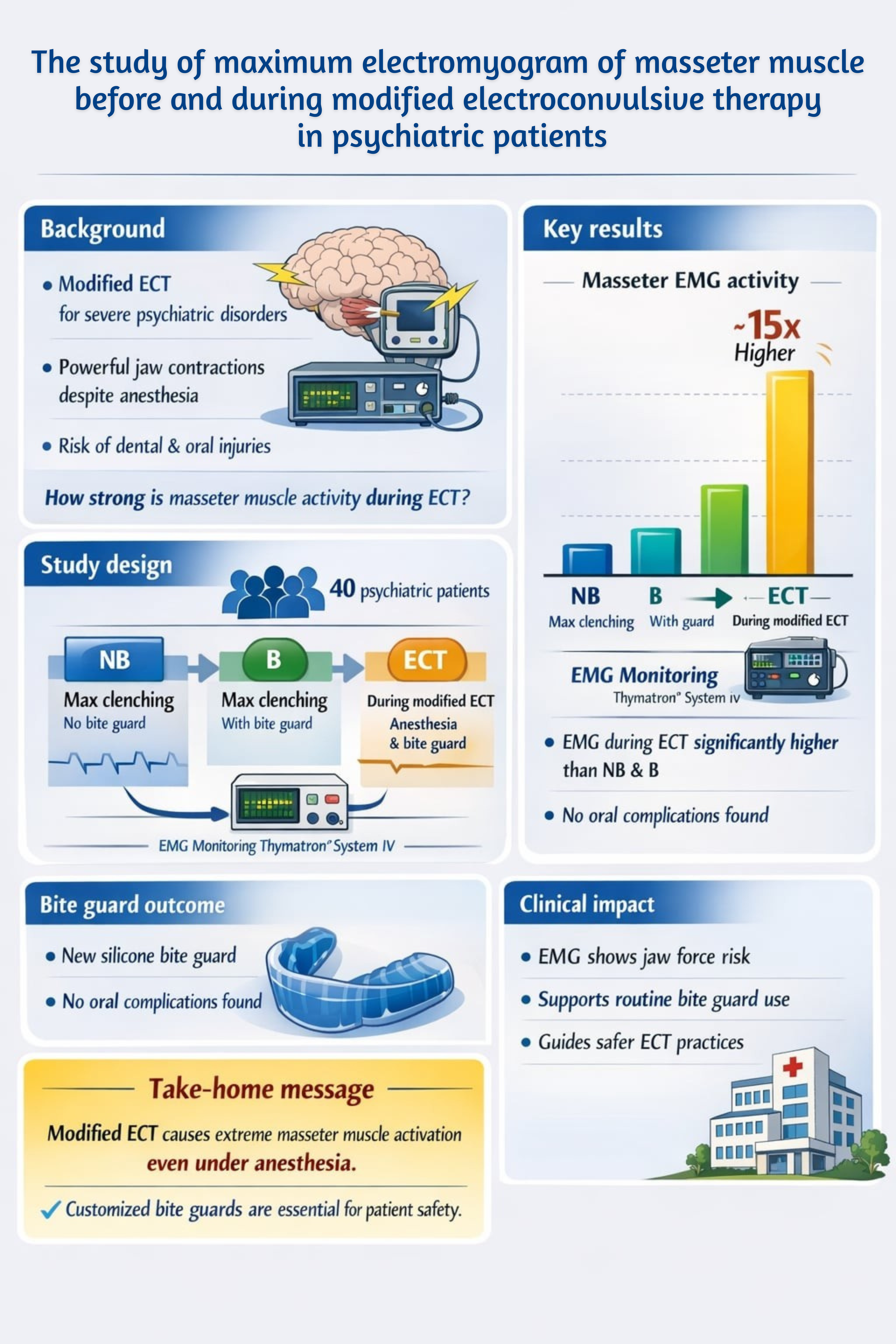
Objectives: To compare the maximum EMG of the masseter muscle under three conditions: 1) maximal clenching without a bite guard, 2) maximal clenching with a bite guard, and 3) during modified ECT with anesthesia, muscle relaxants and a bite guard and to evaluate post procedural oral complications.
Materials and Methods: This cross-sectional study included 40 psychiatric inpatients who undergoing modified ECT at Suanprung Psychiatric Hospital. Surface EMG signals of the masseter muscle were recorded using the Thymatron® System IV (Somatics LLC, USA) under the three conditions: before anesthesia without a bite guard (NB), before anesthesia with a bite guard (B), and during ECT with anesthesia, muscle relaxants and a bite guard (ECT). Differences among conditions were analyzed using repeated measures ANOVA, and independent samples t-tests were used to compare EMG values between groups (<5,451.1 μV vs ≥5,451.1 μV). Significance was set at p<0.05. Post procedural oral examinations were performed to identify any trauma or soft-tissue injuries.
Results: All 40 participants completed the study (mean age 35.63±13.17 years). Schizophrenia was the most prevalent diagnosis (45%), and 67.5% of patients were classified as ASA Class II. The maximum EMG amplitude during ECT was significantly higher than in the NB and B conditions (p<0.001). No significant differences in EMG amplitude were found between the NB and B conditions (p>0.05). Across all participants, EMG values differed significantly among all three conditions (p<0.001). Notably, no oral complications were observed with the use of the newly designed silicone bite guard.
Conclusion: Modified ECT induces significantly higher masseter muscle EMG activity approximately 15-fold greater than pre-ECT clenching. The use of newly designed silicone bite guard effectively prevents oral injury during ECT, supporting its routine clinical application to enhance patient safety and minimize oral complications.
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Personal views expressed by the contributors in their articles are not necessarily those of the Journal of Associated Medical Sciences, Faculty of Associated Medical Sciences, Chiang Mai University.
References
Singh A, Kar SK. How electroconvulsive therapy works?: understanding the neurobiological mechanisms. ClinPsychopharmacol Neurosci. 2017; 15(3): 210-21. doi: 10.9758/cpn.2017.15.3.210.
Saipanit R. Electroconvulsive therapy (ECT). Articles from Ramamental. 2011, accessed 8 December.
Clinical Dental Practice Guideline for Psychiatric Patients 2014 ISBN 978-974-296-825-0.
Jaffe R. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging: a task force report of the American Psychiatric Association. American Journal of Psychiatry. 2002; 159(2): 331. doi.org/10.1176/appi.ajp.159.2.331.
What is electroconvulsive therapy (ECT)? [Internet]. 2023, accessed September 2024.
Ogami S, Yamada M, Kanazawa M, Takeda K, Kimura N, Mizutani H, et al. The effectiveness of a mouth guard to protect against strong occlusion caused by modified electroconvulsive therapy. Dent Traumatol. 2014; 30(5): 368-73. doi: 10.1111/edt.12097.
Muzyka BC, Glass M, Glass OM. Oral health in electroconvulsive therapy: a neglected topic. J ECT. 2017; 33(1): 12-5. doi: 10.1097/YCT.0000000000000351.
Varotto BLR, Neves RRN, Nasri-Heir C, Nápole RCDO, Antequera R, Siqueira JTTd. Mouth guards and intra-oral evaluation for patients. 2021. Rev Bras Odontol. 2021; 78: e1952. doi.org/10.18363/rbo.v78.2021.e1952.
Watts BV, Groft A, Bagian JP, Mills PD. An examination of mortality and other adverse events related to electroconvulsive therapy using a national adverse event report system. J ECT. 2011; 27(2): 105-8. doi: 10.1097/YCT.0b013e3181f6d17f.
Bakke M, MICHLER L, Han K, Möller E. Clinical significance of isometric bite force versus electrical activity in temporal and masseter muscles. Scand J Dent Res. 1989; 97(6): 539-51. doi: 10.1111/j.1600-0722.1989.tb00929.x.
Blanksma N, Van Eijden T, Weijs W. Electromyographic heterogeneity in the human masseter muscle. J Dent Res. 1992; 71(1): 47-52. doi: 10.1177/00220345920710010801.
Van Eijden T, Brugman P, Weijs W, Oosting J. Coactivation of jaw muscles: recruitment order and level as a function of bite force direction and magnitude. J Biomech. 1990; 23(5): 475-85. doi: 10.1016/0021-9290(90)90303-k.
Koolstra J, Van Eijden T. Combined finite-element and rigid-body analysis of human jaw joint dynamics. J Biomech. 2005; 38(12): 2431-9. doi: 10.1016/j.jbiomech.2004.10.014.
Uchida S, Iwasaki L, Marx D, Yotsui Y, Inoue H, Nickel J. Variations in activities of human jaw muscles depend on tooth-tipping moments. Arch Oral Biol. 2008; 53(2): 199-205. doi: 10.1016/j.archoralbio.2007.10.002.
Gonzalez Y, Iwasaki L, McCall Jr W, Ohrbach R, Lozier E, Nickel J. Reliability of electromyographic activity vs. biteforce from human masticatory muscles. ur J Oral Sci. 2011; 119(3): 219-24. doi: 10.1111/j.1600-0722.2011.00823.x
Kongkalai N. Suanprung bite guard for use in electroconvulsive therapy (ECT) in psychiatric patients. Dental Council News. 2020; 3: 26-8.
Kiran S, Bala R, Singh T. Dental protection during modified electroconvulsive therapy using roll-gauze mouth gag. J ECT. 2009; 25(1): 74-5. doi: 10.1097/YCT.0b013e3181770224.
Woo S-W, Do S-H. Tongue laceration during electroconvulsive therapy. Korean J Anesthesiol. 2012; 62(1): 101-2. doi: 10.4097/kjae.2012.62.1.101.
Beli N, Bentham P. Nature and extent of dental pathology and complications arising in patients receiving ECT. Psychiatric Bulletin. 1998; 22(9): 562-5. doi.org/10.1192/pb.22.9.562.
Morris AJ, Roche SA, Bentham P, Wright J. A dental risk management protocol for electroconvulsive therapy. J ECT. 2002;18(2): 84-9. doi: 10.1097/00124509-200206000-00004.
The Practice of ECT: Recommendations for treatment, training and privileging. Convuls Ther. 1990; 6(2): 85-120. PMID: 11659302
Minneman SA. A history of oral protection for the ECT patient: past, present, and future. J ECT. 1995; 11(2): 94-103. PMID: 7552060
Pa parone P, Ee P-L, Kellner CH. Oral protection in electroconvulsive therapy: Modified technique using 2 bite blocks. J ECT. 2019; 35(4): 224. DOI:10.1097/YCT.0000000000000585
Martin D SB. Dental Issues Related to ECT. Cambridge: Cambridge University Press; 2019.
Jirakulsawat A, Siriussawakul A, Triyasunant N, Wangdee A, Jiraroch Y, Chiripu M. Incidence of oral injury and risk factors associated with oral injury in psychiatric patients undergoing electroconvulsive therapy in Siriraj Hospital. Siriraj Med J. 2012; 64(5): 145-8.
Bogdanov V. Type of correlation between bite force and EMG activity of the temporalis and masseter muscles during maximal and submaximal clenching. Folia Med. 2023; 65(6): 975-85. doi: 10.3897/folmed.65.e107180.
