
ภาวะเลือดเป็นกรดจากการคั่งของกรดแลคติกจากการใช้ยาเทอร์บูทาลีนในผู้ป่วยตั้งครรภ์ที่มีภาวะเจ็บครรภ์คลอดก่อนกำหนด: รายงานผู้ป่วยและทบทวนวรรณกรรม
Article Sidebar
Main Article Content
บทคัดย่อ
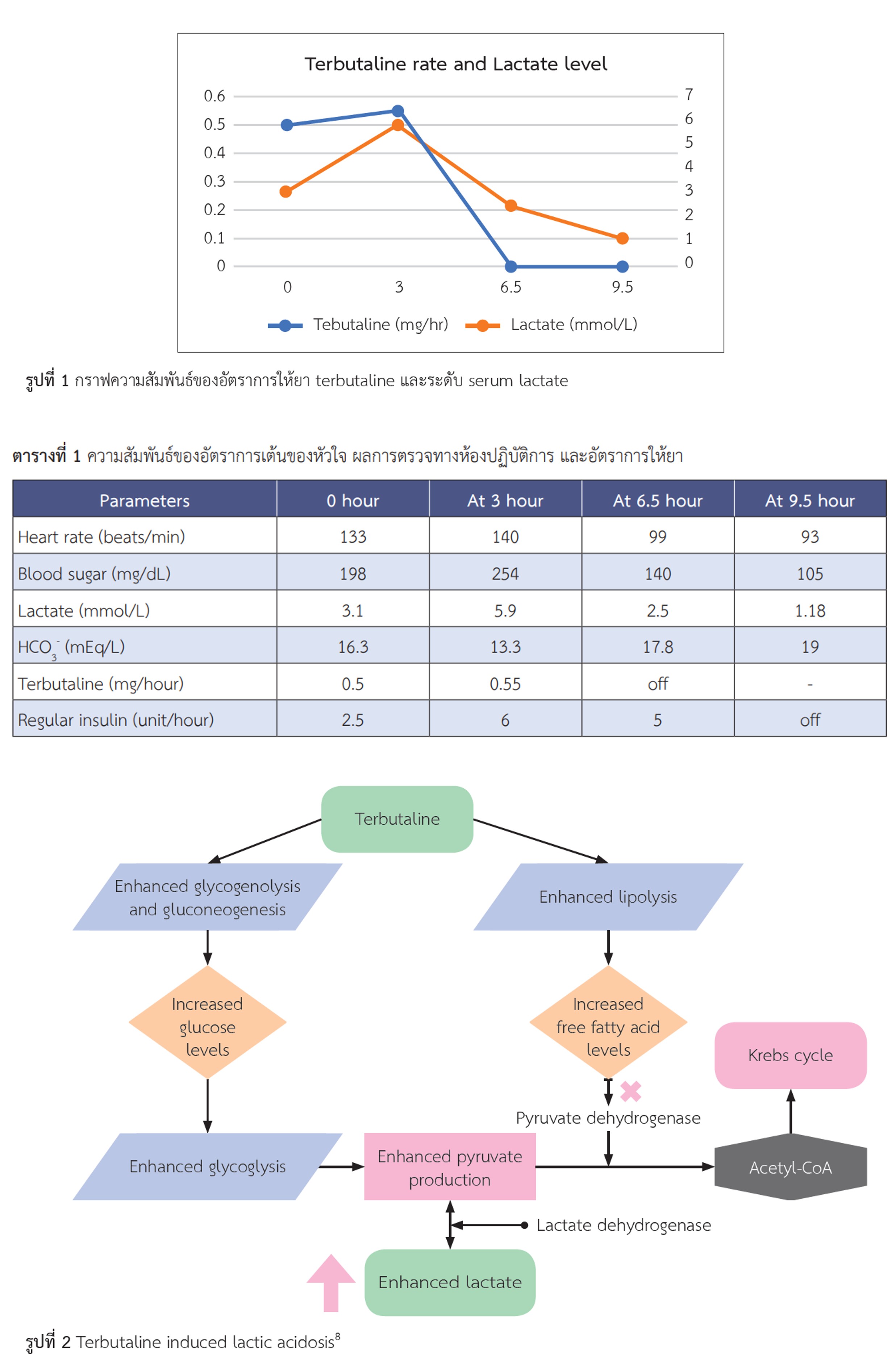
ภาวะเจ็บครรภ์คลอดก่อนกำหนดเป็นภาวะที่พบบ่อยในเวชปฏิบัติ ภาวะเจ็บครรภ์คลอดก่อนกำหนดมีนิยาม คือ ภาวะที่มดลูกบีบตัวอย่างสม่ำเสมอ ร่วมกับมีการเปลี่ยนแปลงของปากช่องคลอดที่เกิดในอายุครรภ์ 20+ 07/ สัปดาห์ ถึง 36+ 67/ สัปดาห์ ภาวะคลอดก่อนกำหนดเป็นสาเหตุสำคัญของภาวะเจ็บป่วยและการเสียชีวิตของทารกแรกเกิด กรณีคลอดที่อายุครรภ์ก่อน 34 สัปดาห์ ระบบทางเดินหายใจของทารกในครรภ์ยังเจริญเติบโตไม่เต็มที่ จึงมีความจำเป็นที่ต้องรักษาด้วยยาคอร์ติโคสเตียรอยด์ชนิดฉีดเข้าทางกล้ามเนื้อ จากภาวะดังกล่าวจึงได้มีการนำยามาใช้ในการยับยั้งไม่ให้มดลูกหดรัดตัวเพื่อรอระยะเวลาของการให้ยาคอร์ติโคสเตียรอยออกฤทธิ์ เช่น ยากลุ่ม calcium-channel blockers และ ยากลุ่ม beta-adrenergic receptor agonists เป็นต้น รายงานผู้ป่วยนี้ กล่าวถึงผู้หญิงที่มาด้วยอาการเจ็บครรภ์คลอดก่อนกำหนดที่ได้รับการรักษาด้วยยาเทอร์บูทาลีน (terbutaline) โดยระหว่างได้รับยา ผู้ป่วยเกิดภาวะเลือดเป็นกรดเมแทบอลิก (metabolic acidosis) จากผลการตรวจทางห้องปฏิบัติการสรุปได้ว่ามีสาเหตุมาจากการคั่งของกรดแลคติก (lactic acidosis) ที่เกิดจากการใช้ยาเทอร์บูทาลีน หลังจากหยุดยาพบว่าภาวะเลือดเป็นกรดจากการคั่งของกรดแลคติกดีขึ้นและหายไป ในการวินิจฉัยจำเป็นต้องค้นหาสาเหตุอื่นก่อน ในกรณีที่ไม่พบสาเหตุอื่น ๆ ร่วมกับการที่ภาวะเลือดเป็นกรดจากการคั่งของกรดแลคติกหายไปหลังหยุดใช้ยา จึงช่วยให้สามารถสรุปได้ว่าเป็นภาวะเลือดเป็นกรดจากการคั่งของกรดแลคติกจากการใช้ยาเทอร์บูทาลีน ในส่วนของกลไกมีรายงานว่ายาเทอร์บูทาลีน ไปเพิ่มกระบวนการไกลโคไลซิสส่งผลให้ไพรูเวทและแลคเตทเพิ่มสูงขึ้น
Article Details

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
บทความนี้ตีพิมพ์ภายไต้การอนุญาต CC BY-NC-ND 4.0 ซึ่งอนุญาตให้สามารถใช้บทความนี้พื่อวัตถุประสงค์ใดๆ ก็ตามที่ไม่ใช่เชิงพาณิชย์ โดยต้องมีการอ้างถึงที่มาของบทความอย่างครบถ้วน ใครก็ตามสามารถคัดลอกและแจกจ่ายทุกส่วนของบทความนี้โดยไม่ต้องขออนุญาตจากผู้ประพันธ์หรือสมาคมโรคไตแห่งประเทศไทย
เอกสารอ้างอิง
Beck S, Wojdyla D, Say L, Betran AP, Merialdi M, Requejo JH, et al. The worldwide incidence of preterm birth: a systematic review of maternal mortality and morbidity. Bull World Health Organ. 2010;88(1):31–8.
Goldenberg RL, Culhane JF, Iams JD, Romero R. Epidemiology and causes of preterm birth. Lancet Lond Engl. 2008;371(9606):75–84.
American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics. Practice Bulletin No. 171: Management of Preterm Labor. Obstet Gynecol. 2016;128(4):e155-64.
Roberts D, Dalziel S. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev. 2006;(3):CD004454.
Hearne AE, Nagey DA. Therapeutic agents in preterm labor: tocolytic agents. Clin Obstet Gynecol. 2000;43(4):787–801.
Desir D, Van Coevorden A, Kirkpatrick C, Caufriez A. Ritodrineinduced acidosis in pregnancy. Br Med J. 1978;2(6146):1194.
Phoophiboon V, Singhagowinta P, Boonkaya S, Sriprasart T. Salbutamol-induced lactic acidosis in status asthmaticus survivor. BMC Pulm Med. 2021;21(1):23.
Kraut JA, Madias NE. Lactic acidosis. N Engl J Med. 2014;371(24):2309–19.
Liedtke AG, Lava SAG, Milani GP, Agostoni C, Gilardi V, Bianchetti MG, et al. Selective ß2-Adrenoceptor Agonists and Relevant Hyperlactatemia: Systematic Review and Meta-Analysis. J Clin Med. 2019;9(1):71.
Haas DM, Imperiale TF, Kirkpatrick PR, Klein RW, Zollinger TW, Golichowski AM. Tocolytic therapy: a meta-analysis and decision analysis. Obstet Gynecol. 2009;113(3):585–94.
Dagklis T, Akolekar R, Villalain C, Tsakiridis I, Kesrouani A, Tekay A, et al. Management of preterm labor: Clinical practice guideline and recommendation by the WAPM-World Association of Perinatal Medicine and the PMF-Perinatal Medicine Foundation. Eur J Obstet Gynecol Reprod Biol. 2023;291:196–205.
Haas DM, Benjamin T, Sawyer R, Quinney SK. Short-term tocolytics for preterm delivery – current perspectives. Int J Womens Health. 2014;6:343–9.
Yu ASL, Chertow GM, Luyckx VA, Marsden PA, Skorecki K, Taal MW, editors. Brenner & Rector’s the kidney [Internet]. Eleventh edition. Philadelphia, PA: Elsevier; 2020 [cited 2023 Dec 10].2677 p. Available from: https://www.clinicalkey.com.au/dura/browse/bookChapter/3-s2.0-C20161038580
Adam K, Ou CN, Cotton DB. Combined effect of terbutaline and betamethasone on glucose homeostasis in preterm labor. Fetal Diagn Ther. 1993;8(3):187–94.
Braden GL, Oeyen PT von, Germain MJ, Watson DJ, Haag BL. Ritodrine- and terbutaline-induced hypokalemia in preterm labor: Mechanisms and consequences. Kidney Int. 1997;51(6):1867–75.
Richards SR, Chang FE, Stempel LE. Hyperlactacidemia associated with acute ritodrine infusion. Am J Obstet Gynecol. 1983;146(1):1–5.
Kirkpatrick C, Quenon M, Desir D. Blood anions and electrolytes during ritodrine infusion in preterm labor. Am J Obstet Gynecol. 1980;138(5):523–7.
Cotton DB, Strassner HT, Lipson LG, Goldstein DA. The effects of terbutaline on acid base, serum electrolytes, and glucose homeostasis during the management of pre term labor. Am J Obstet Gynecol. 1981;141(5):617–24.
Najout H, Moutawakil M, Elkoundi A, Doghmi N, Bekkali H. Salbutamol-induced severe lactic acidosis in acute asthma. SAGE Open Med Case Rep. 2020;8:2050313X20969027.
Meegada S, Muppidi V, Siddamreddy S, Challa T, Katta SK. Albuterol-Induced Type B Lactic Acidosis: Not an Uncommon Finding. Cureus. 2020;12(5):e8269.
Rodrigo G, Rodrigo C. Elevated plasma lactate level associated with high dose inhaled albuterol therapy in acute severe asthma. Emerg Med J EMJ. 2005;22(6):404–8.
Lau E, Mazer J, Carino G. Inhaled β-agonist therapy and respiratory muscle fatigue as under-recognised causes of lactic acidosis. Case Rep. 2013;2013:bcr2013201015.
Dodda VR, Spiro P. Can albuterol be blamed for lactic acidosis? Respir Care. 2012;57(12):2115–8.
Sharif Z, Al-Alawi M. Beware of beta! A case of salbutamolinduced lactic acidosis in severe asthma. Case Rep. 2018;2018:bcr.
Prakash S, Mehta S. Lactic acidosis in asthma: report of two cases and review of the literature. Can Respir J. 2002;9(3):203–8.
Sturney S, Suntharalingam J. Treating acute asthma – salbutamol may not always be the right answer. Clin Med. 2012;12(2):181–2.
Assessment UENC for E. Lactic acidosis as a complication of β-adrenergic aerosols [Internet]. 2009 [cited 2023 Nov 28]. Available from: https://hero.epa.gov/hero/index.cfm/reference/details/reference_id/2572404
Claret PG, Bobbia X, Boutin C, Rougier M, de la Coussaye JE. Lactic acidosis as a complication of β-adrenergic aerosols. Am J Emerg Med. 2012;30(7):1319.e5-6.
Manthous CA. Lactic acidosis in status asthmaticus : three cases and review of the literature. Chest. 2001;119(5):1599–602.
Chasiotis D, Sahlin K, Hultman E. Regulation of glycogenolysis in human muscle in response to epinephrine infusion. J Appl Physiol. 1983;54(1):45–50.
