
การศึกษาแบบทดลองสุ่มถึงผลของยา Empagliflozin/Linagliptin ต่อภาวะ Oxidative Stress ในผู้ป่วยโรคไตเรื้อรังจากเบาหวาน
Article Sidebar
Main Article Content
บทคัดย่อ
บทนำ: การรักษาด้วยยา sodium-glucose cotransporter 2 inhibitors (SGLT2i) และ dipeptidyl peptidase-4 inhibitors (DPP-4i) คาดว่าช่วยเสริมฤทธิ์ในการควบคุมระดับน้ำตาลในเลือด และ ลดภาวะ reactive oxygen species (ROS) ในผู้ป่วยเบาหวานชนิดที่ 2 การศึกษานี้จึงประเมินผลขของยา SGLT2i ร่วมกับ DPP-4i เพื่อลดภาวะ oxidative stress ภายในไตจากภาวะน้ำตาลในเลือดสูง
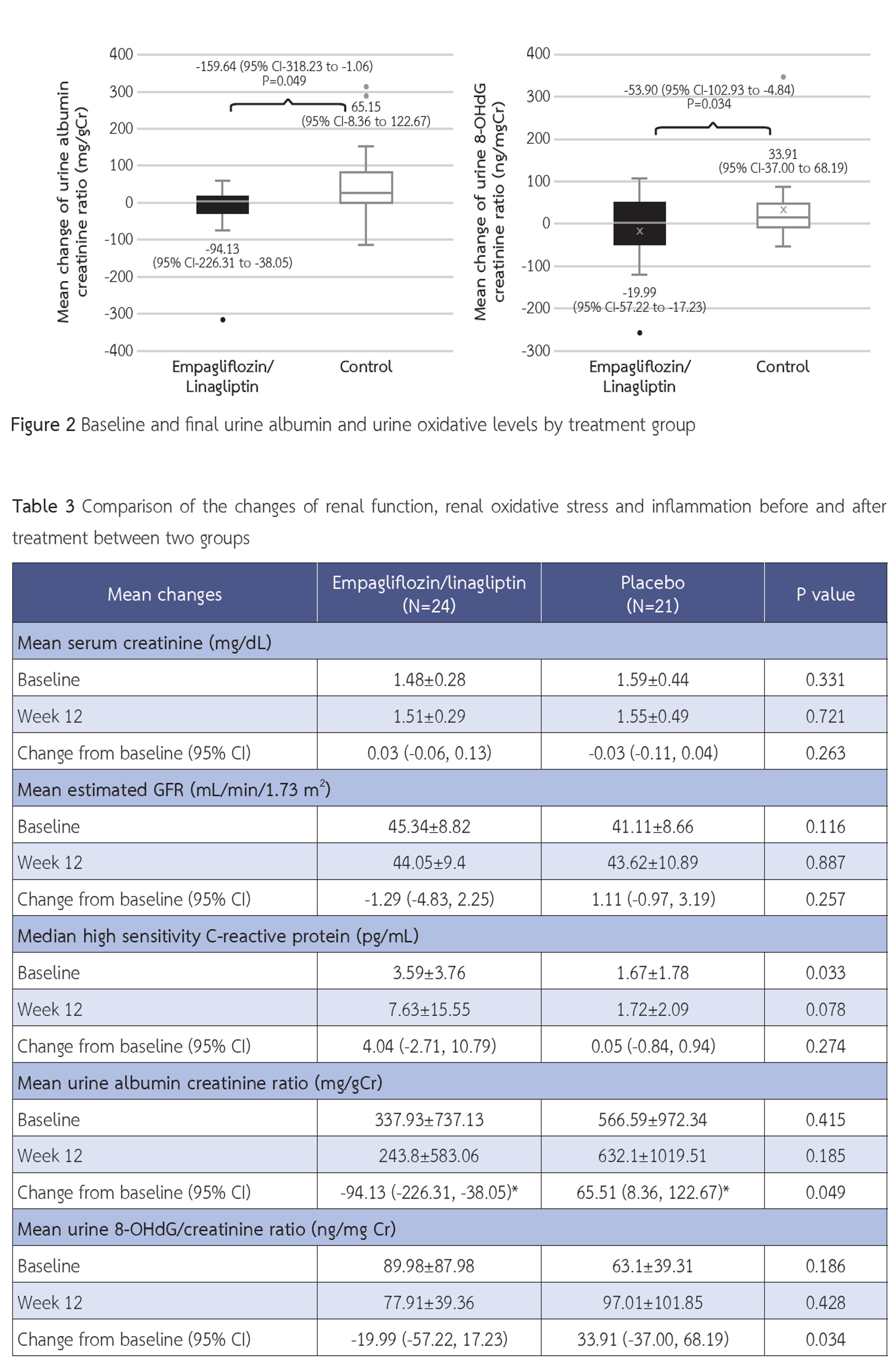
ระเบียบวิธีวิจัย: การศึกษาในผู้ป่วยเบาหวานชนิดที่ 2 ที่มีโรคไตเรื้อรังระยะที่ 3 โดยทดลองสุ่มให้ยา empagliflozin 10 มก./วัน ร่วมกับ linagliptin 5 มก./วัน เทียบกับการรักษามาตรฐานเป็นเวลา 12 สัปดาห์ แล้วประเมินภาวะ oxidative stress ภายในไตจากการตรวจวัด 8-hydroxy-2’-deoxyguanosine (8-OHdG) และแอลบูมินต่อครีแอทินินในปัสสาวะ
ผลการวิจัย: ผู้ป่วยจำนวน 48 รายเข้าร่วมการศึกษา หลังการรักษา 12 สัปดาห์ กลุ่มที่ได้รับ empagliflozin/linagliptin สามารถลดระดับ 8-OHdG ในปัสสาวะอย่างมีนัยสำคัญทางสถิติเมื่อเทียบกับกลุ่มควบคุม นอกจากนี้กลุ่มที่ได้รับ empagliflozin/linagliptin สามารถลดระดับแอลบูมินในปัสสาวะอย่างมีนัยสำคัญทางสถิติเมื่อเทียบกับกลุ่มควบคุม และสามารถลดระดับน้ำตาลสะสมในเลือดอย่างมีนัยสำคัญทางสถิติเมื่อเทียบกับกลุ่มควบคุมเช่นกัน โดยไม่พบความแตกต่างกันของน้ำหนักตัว ความดันโลหิตและการทำงานของไตระหว่างผู้ป่วยทั้งสองกลุ่ม ผลข้างเคียงจากการรักษาในผู้ป่วยทั้งสองกลุ่มไม่มีความแตกต่างกัน รวมถึงการเกิดภาวะน้ำตาลในเลือดต่ำ
สรุป: การใช้ยา SGLT2i และ DPP-4i ร่วมกันเป็นระยะเวลา 12 สัปดาห์ สามารถเพื่อลดภาวะ oxidative stress ภายในไต และ ระดับน้ำตาลในเลือดในผู้ป่วยโรคไตเรื้อรังจากเบาหวาน ซึ่งอาจช่วยชะลอการไตเสื่อมจากโรคเบาหวาน โดยผู้ป่วยสามารถทนต่อการรักษาได้ดี
Article Details

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
บทความนี้ตีพิมพ์ภายไต้การอนุญาต CC BY-NC-ND 4.0 ซึ่งอนุญาตให้สามารถใช้บทความนี้พื่อวัตถุประสงค์ใดๆ ก็ตามที่ไม่ใช่เชิงพาณิชย์ โดยต้องมีการอ้างถึงที่มาของบทความอย่างครบถ้วน ใครก็ตามสามารถคัดลอกและแจกจ่ายทุกส่วนของบทความนี้โดยไม่ต้องขออนุญาตจากผู้ประพันธ์หรือสมาคมโรคไตแห่งประเทศไทย
เอกสารอ้างอิง
Nata N, Rangsin R, Supasyndh O, Satirapoj B. Impaired Glomerular Filtration Rate in Type 2 Diabetes Mellitus Subjects: A Nationwide Cross-Sectional Study in Thailand. J Diabetes Res. 2020;2020:6353949.
Afkarian M, Sachs MC, Kestenbaum B, Hirsch IB, Tuttle KR, Himmelfarb J, et al. Kidney disease and increased mortality risk in type 2 diabetes. J Am Soc Nephrol. 2013;24(2):302-8.
Ruospo M, Saglimbene VM, Palmer SC, De Cosmo S, Pacilli A, Lamacchia O, et al. Glucose targets for preventing diabetic kidney disease and its progression. Cochrane Database Syst Rev. 2017;6(6):CD010137.
Lo C, Toyama T, Wang Y, Lin J, Hirakawa Y, Jun M, et al. Insulin and glucose-lowering agents for treating people with diabetes and chronic kidney disease. Cochrane Database Syst Rev. 2018;9(9):CD011798.
Satirapoj B, Pratipanawatr T, Ongphiphadhanakul B, Suwanwalaikorn S, Benjasuratwong Y, Nitiyanant W. Real-world Evaluation of glycemic control and hypoglycemic Events among type 2 Diabetes mellitus study (REEDS): a multicentre, crosssectional study in Thailand. BMJ Open. 2020;10(2):e031612.
Bonora BM, Avogaro A, Fadini GP. Extraglycemic Effects of SGLT2 Inhibitors: A Review of the Evidence. Diabetes Metab Syndr Obes. 2020;13:161-74.
Duni A, Liakopoulos V, Roumeliotis S, Peschos D, Dounousi E. Oxidative Stress in the Pathogenesis and Evolution of Chronic Kidney Disease: Untangling Ariadne’s Thread. Int J Mol Sci. 2019;20(15).
Yaribeygi H, Butler AE, Atkin SL, Katsiki N, Sahebkar A. Sodiumglucose cotransporter 2 inhibitors and inflammation in chronic kidney disease: Possible molecular pathways. J Cell Physiol. 2018;234(1):223-30.
Aroor AR, Sowers JR, Jia G, DeMarco VG. Pleiotropic effects of the dipeptidylpeptidase-4 inhibitors on the cardiovascular system. Am J Physiol Heart Circ Physiol. 2014;307(4):H477-92.
Ishibashi Y, Matsui T, Maeda S, Higashimoto Y, Yamagishi S. Advanced glycation end products evoke endothelial cell damage by stimulating soluble dipeptidyl peptidase-4 production and its interaction with mannose 6-phosphate/insulin-like growth factor II receptor. Cardiovasc Diabetol. 2013;12:125.
Garvey WT, Van Gaal L, Leiter LA, Vijapurkar U, List J, Cuddihy R, et al. Effects of canagliflozin versus glimepiride on adipokines and inflammatory biomarkers in type 2 diabetes. Metabolism. 2018;85:32-7.
Shigiyama F, Kumashiro N, Miyagi M, Ikehara K, Kanda E, Uchino H, et al. Effectiveness of dapagliflozin on vascular endothelial function and glycemic control in patients with early-stage type 2 diabetes mellitus: DEFENCE study. Cardiovasc Diabetol. 2017;16(1):84.
Niedowicz DM, Daleke DL. The role of oxidative stress in diabetic complications. Cell Biochem Biophys. 2005;43(2):289-330.
Suzuki D, Miyata T, Saotome N, Horie K, Inagi R, Yasuda Y, et al. Immunohistochemical evidence for an increased oxidative stress and carbonyl modification of proteins in diabetic glomerular lesions. J Am Soc Nephrol. 1999;10(4):822-32.
Shin CS, Moon BS, Park KS, Kim SY, Park SJ, Chung MH, et al. Serum 8-hydroxy-guanine levels are increased in diabetic patients. Diabetes Care. 2001;24(4):733-7.
Schei J, Fuskevag OM, Stefansson VTN, Solbu MD, Jenssen TG, Eriksen BO, et al. Urinary Markers of Oxidative Stress Are Associated With Albuminuria But Not GFR Decline. Kidney Int Rep. 2018;3(3):573-82.
Chadha M, Das AK, Deb P, Gangopadhyay KK, Joshi S, Kesavadev J, et al. Expert Opinion: Optimum Clinical Approach to Combination-Use of SGLT2i + DPP4i in the Indian Diabetes Setting. Diabetes Ther. 2022;13(5):1097-114.
Nakashima S, Matsui T, Takeuchi M, Yamagishi SI. Linagliptin blocks renal damage in type 1 diabetic rats by suppressing advanced glycation end products-receptor axis. Horm Metab Res. 2014;46(10):717-21.
Ashrafi Jigheh Z, Ghorbani Haghjo A, Argani H, Roshangar L, Rashtchizadeh N, Sanajou D, et al. Empagliflozin alleviates renal inflammation and oxidative stress in streptozotocin-induced diabetic rats partly by repressing HMGB1-TLR4 receptor axis. Iran J Basic Med Sci. 2019;22(4):384-90.
Lee YH, Kim SH, Kang JM, Heo JH, Kim DJ, Park SH, et al. Empagliflozin attenuates diabetic tubulopathy by improving mitochondrial fragmentation and autophagy. Am J Physiol Renal Physiol. 2019;317(4):F767-F80.
Das NA, Carpenter AJ, Belenchia A, Aroor AR, Noda M, Siebenlist U, et al. Empagliflozin reduces high glucose-induced oxidative stress and miR-21-dependent TRAF3IP2 induction and RECK suppression, and inhibits human renal proximal tubular epithelial cell migration and epithelial-to-mesenchymal transition. Cell Signal. 2020;68:109506.
Korbut AI, Taskaeva IS, Bgatova NP, Muraleva NA, Orlov NB, Dashkin MV, et al. SGLT2 Inhibitor Empagliflozin and DPP4 Inhibitor Linagliptin Reactivate Glomerular Autophagy in db/db Mice, a Model of Type 2 Diabetes. Int J Mol Sci. 2020;21(8).
Makino H, Matsuo M, Hishida A, Koezuka R, Tochiya M, Ohata Y, et al. Effect of linagliptin on oxidative stress markers in patients with type 2 diabetes: a pilot study. Diabetol Int. 2019;10(2):148-52.
Wanner C, Inzucchi SE, Lachin JM, Fitchett D, von Eynatten M, Mattheus M, et al. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N Engl J Med. 2016;375(4):323-34.
Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N Engl J Med. 2019;380(24):2295-306.
Mosenzon O, Wiviott SD, Cahn A, Rozenberg A, Yanuv I, Goodrich EL, et al. Effects of dapagliflozin on development and progression of kidney disease in patients with type 2 diabetes: an analysis from the DECLARE-TIMI 58 randomised trial. Lancet Diabetes Endocrinol. 2019;7(8):606-17.
Mosenzon O, Leibowitz G, Bhatt DL, Cahn A, Hirshberg B, Wei C, et al. Effect of Saxagliptin on Renal Outcomes in the SAVOR-TIMI 53 Trial. Diabetes Care. 2017;40(1):69-76.
Rosenstock J, Perkovic V, Johansen OE, Cooper ME, Kahn SE, Marx N, et al. Effect of Linagliptin vs Placebo on Major Cardiovascular Events in Adults With Type 2 Diabetes and High Cardiovascular and Renal Risk: The CARMELINA Randomized Clinical Trial. JAMA. 2019;321(1):69-79.
Kanasaki K, Shi S, Kanasaki M, He J, Nagai T, Nakamura Y, et al. Linagliptin-mediated DPP-4 inhibition ameliorates kidney fibrosis in streptozotocin-induced diabetic mice by inhibiting endothelial-to-mesenchymal transition in a therapeutic regimen. Diabetes. 2014;63(6):2120-31.
Birnbaum Y, Bajaj M, Yang HC, Ye Y. Combined SGLT2 and DPP4 Inhibition Reduces the Activation of the Nlrp3/ASC Inflammasome and Attenuates the Development of Diabetic Nephropathy in Mice with Type 2 Diabetes. Cardiovasc Drugs Ther. 2018;32(2):135-45.
Rizos CV, Filippatos TD, Elisaf MS. Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes. Expert Opin Drug Metab Toxicol. 2018;14(1):117-25.
Cho YK, Kang YM, Lee SE, Lee J, Park JY, Lee WJ, et al. Efficacy and safety of combination therapy with SGLT2 and DPP4 inhibitors in the treatment of type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab. 2018;44(5):393-401.
Lewin A, DeFronzo RA, Patel S, Liu D, Kaste R, Woerle HJ, et al. Initial combination of empagliflozin and linagliptin in subjects with type 2 diabetes. Diabetes Care. 2015;38(3):394-402.
Watada H, Yamauchi T, Yamamoto F, Taniguchi A, Yarush L, Heilmann C, et al. Safety and tolerability of empagliflozin and linagliptin combination therapy in patients with type 2 diabetes mellitus: a pooled analysis of data from five randomized, controlled clinical trials. Expert Opin Drug Saf. 2020;19(9):1193-202.
