
ปัจจัยทำนายและผลลัพธ์ของภาวะความเข้มข้นเลือดเพิ่มสูงขึ้นหลังได้รับยา Sodium-Glucose Cotransporter-2 Inhibitors ในผู้ป่วยโรคเบาหวานชนิดที่ 2
Article Sidebar
Main Article Content
บทคัดย่อ
บทนำ: จากการศึกษาพบว่ายากลุ่ม Sodium-Glucose Cotransporter-2 Inhibitors (SGLT2i) อาจทำให้ความเข้มข้นของเลือดสูงขึ้นได้ ความเข้มข้นเลือดที่สูงขึ้นนี้อาจส่งผลดีต่อผู้ป่วยทั้งทางระบบหัวใจและหลอดเลือดและระบบไต การศึกษานี้มีวัตถุประสงค์เพื่อศึกษาการเปลี่ยนแปลงของความเข้มข้นเลือด ความชุกและปัจจัยทำนายการเกิดภาวะความเข้มข้นเลือดเพิ่มสูงขึ้น (erythrocytosis) และเปรียบเทียบการเกิดผลลัพธ์ต่อระบบหัวใจและหลอดเลือดและไต ระหว่างกลุ่มผู้ป่วยที่มีภาวะความเข้มข้นเลือดเพิ่มสูงขึ้นกับกลุ่มที่ไม่พบ
ภาวะดังกล่าว ในผู้ป่วยโรคเบาหวานชนิดที่ 2 หลังจากได้รับยา SGLT2i
ระเบียบวิธีวิจัย: การศึกษาแบบย้อนหลังระหว่างเดือนมกราคม 2563 – ธันวาคม 2565 ในผู้ป่วยโรคเบาหวานชนิดที่ 2 ที่ได้รับยาในกลุ่ม SGLT2i ติดต่อกันนานมากกว่า 3 เดือน โดยมีการเก็บข้อมูลระดับฮีโมโกลบิน และ/หรือ ฮีมาโตคริต ก่อนให้การรักษา และ 3-12 เดือน หลังจากได้รับยาไปจนกระทั่งสิ้นสุดการศึกษา ผู้ป่วยที่มีการเพิ่มขึ้นของฮีโมโกลบิน ≥2 มิลลิกรัม/เดซิลิตร จากก่อนการรักษา ถือว่ามีภาวะความเข้มข้นเลือดเพิ่มสูงขึ้น
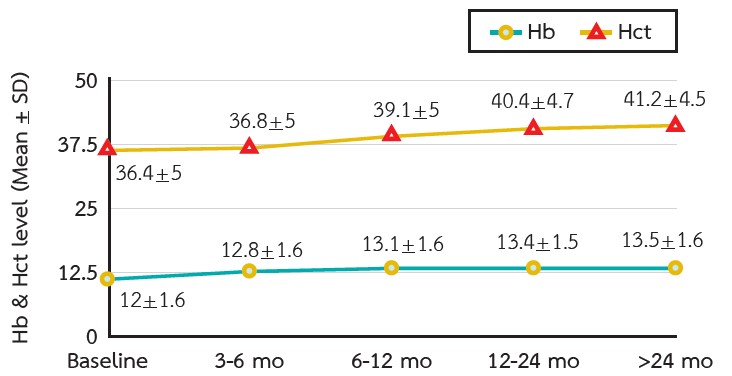
ผลการศึกษา: มีผู้ที่ผ่านเกณฑ์การคัดเข้าและออกจำนวนทั้งหมด 336 คน หลังได้รับยา SGLT2i พบว่าความเข้มข้นเลือดมีการเพิ่มขึ้นตามระยะเวลาที่ผ่านไป โดยมีค่ามัธยฐานของการเพิ่มขึ้นของฮีโมโกลบินอยู่ที่ 0.7, 1, 1.3, 1.5 กรัม/เดซิลิตร ที่ระยะเวลา 3, 6, 12, >24 เดือนตามลำดับ มีผู้ป่วยที่เข้าข่ายภาวะความเข้มข้นเลือดเพิ่มสูงขึ้นร้อยละ 37.2 ปัจจัยที่ทำนายภาวะความเข้มข้นเลือดเพิ่มสูงขึ้น ได้แก่ อายุมากกว่า 60 ปี, เป็นโรคไตเรื้อรัง, ได้รับยาขับปัสสาวะกลุ่ม thiazide และ ยา beta-blockers, มีค่าฮีโมโกลบินและอัตราการกรองของไตตั้งต้นต่ำ ในขณะที่ไม่พบความสัมพันธ์ระหว่างภาวะความเข้มข้นเลือดเพิ่มสูงขึ้นกับผลลัพธ์ต่อระบบหัวใจและหลอดเลือดและระบบไต
สรุป: ฮีโมโกลบินมีระดับเพิ่มขึ้นเรื่อย ๆ ในผู้ป่วยเบาหวานชนิดที่ 2 หลังได้รับการรักษาด้วย SGLT2i โดยพบความชุกของภาวะความเข้มข้นเลือดเพิ่มสูงขึ้นที่ค่อนข้างสูง ในขณะที่ไม่พบความสัมพันธ์ระหว่างภาวะดังกล่าวกับผลลัพธ์ของระบบหัวใจและหลอดเลือดและระบบไต
Article Details

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
บทความนี้ตีพิมพ์ภายไต้การอนุญาต CC BY-NC-ND 4.0 ซึ่งอนุญาตให้สามารถใช้บทความนี้พื่อวัตถุประสงค์ใดๆ ก็ตามที่ไม่ใช่เชิงพาณิชย์ โดยต้องมีการอ้างถึงที่มาของบทความอย่างครบถ้วน ใครก็ตามสามารถคัดลอกและแจกจ่ายทุกส่วนของบทความนี้โดยไม่ต้องขออนุญาตจากผู้ประพันธ์หรือสมาคมโรคไตแห่งประเทศไทย
เอกสารอ้างอิง
Vejakama P, Ingsathit A, Attia J, Thakkinstian A. Epidemiological Study of Chronic Kidney Disease Progression: A Large-Scale Population-Based Cohort Study. Medicine (Baltimore). 2015;94(4):e475.
Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH, et al. Effects of Losartan on Renal and Cardiovascular Outcomes in Patients with Type 2 Diabetes and Nephropathy. N Engl J Med. 2001;345(12):861–9.
Rodby RA, Rohde RD, Clarke WR, Hunsicker LG, Anzalone DA, Atkins RC, et al. The Irbesartan Type II Diabetic Nephropathy Trial: study design and baseline patient characteristics. Nephrol Dial Transplant. 2000;15(4):487–97.
Cheungpasitporn W, Thongprayoon C, Chiasakul T, Korpaisarn S, Erickson SB. Renin-angiotensin system inhibitors linked to anemia: a systematic review and meta-analysis. QJM. 2015;108(11):879–84.
Kendrick J, Chonchol MB. Nontraditional risk factors for cardiovascular disease in patients with chronic kidney disease. Nat Clin Pract Nephrol. 2008;4(12):672–81.
Washburn WN, Poucher SM. Differentiating sodiumglucose co-transporter-2 inhibitors in development for the treatment of type 2 diabetes mellitus. Expert Opin Investig Drugs. 2013;22(4):463-86.
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med. 2015;373(22):2117–28.
The EMPA-KIDNEY Collaborative Group, Herrington WG, Staplin N, Wanner C, Green JB, Hauske SJ, et al. Empagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2023;388(2):117–27.
Heerspink HJL, Stefánsson BV, Correa-Rotter R, Chertow GM, Greene T, Hou FF, et al. Dapagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2020;383(15):1436–46.
Rossing P, Caramori ML, Chan JCN, Heerspink HJL, Hurst C, Khunti K, et al. KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int. 2022;102(5S):S1-S127.
American Diabetes Association. Standards of Medical Care in Diabetes—2022 Abridged for Primary Care Providers. Clin Diabetes. 2022;40(1):10–38.
Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2019;380(4):347–57.
Wang X, Fu R, Liu H, Ma Y, Qiu X, Dong Z. The effects of sodium glucose co-transporter (SGLT) 2 inhibitors on hematocrit levels: a systematic review and metaanalysis of randomized controlled trials. Ann Palliat Med. 2021;10(6):6467-81.
Levin A, Thompson CR, Ethier J, Carlisle EJ, Tobe S, Mendelssohn D, et al. Left ventricular mass index increase in early renal disease: impact of decline in hemoglobin. Am J Kidney Dis. 1999;34(1):125–34.
Marathias KP, Lambadiari VA, Markakis KP, Vlahakos VD, Bacharaki D, Raptis AE, et al. Competing Effects of Renin Angiotensin System Blockade and Sodium-Glucose Cotransporter-2 Inhibitors on Erythropoietin Secretion in Diabetes. Am J Nephrol. 2020;51(5):349–56.
Souma T, Suzuki N, Yamamoto M. Renal erythropoietinproducing cells in health and disease. Front Physiol. 2015;6:167.
Souma T, Nezu M, Nakano D, Yamazaki S, Hirano I, Sekine H, et al. Erythropoietin Synthesis in Renal Myofibroblasts Is Restored by Activation of Hypoxia Signaling. J Am Soc Nephrol. 2016;27(2):428–38.
Ghanim H, Abuaysheh S, Hejna J, Green K, Batra M, Makdissi A, et al. Dapagliflozin Suppresses Hepcidin And Increases Erythropoiesis. J Clin Endocrinol Metab. 2020;105(4):dgaa057.
Tilg H, Moschen AR. Inflammatory Mechanisms in the Regulation of Insulin Resistance. Mol Med. 2008;14(3–4):222–31.
Fleming RE. Iron and inflammation: cross-talk between pathways regulating hepcidin. J Mol Med (Berl). 2008;86(5):491–4.
Mithoowani S, Laureano M, Crowther MA, Hillis CM. Investigation and management of erythrocytosis. CMAJ. 2020;192(32):E913–8.
Gašperšič J, Kristan A, Kunej T, Zupan IP, Debeljak N. Erythrocytosis: genes and pathways involved in disease development. Blood Transfus. 2021;19(6):518–32.
Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–91.
Sano M, Goto S. Possible Mechanism of Hematocrit Elevation by Sodium Glucose Cotransporter 2 Inhibitors and Associated Beneficial Renal and Cardiovascular Effects. Circulation. 2019;139(17):1985–7.
