
การศึกษาประสิทธิภาพของแมกนีเซียมเสริมต่อการทำงานของเซลล์เยื่อบุผนังหลอดเลือดในผู้ป่วยโรคไตเรื้อรังระยะ ๔, การศึกษาแบบสุ่ม
Article Sidebar
Main Article Content
บทคัดย่อ
บทนำ: ภาวะผิดปกติของเซลล์เยื่อบุผนังหลอดเลือดมีความสัมพันธ์กับภาวะแทรกซ้อนทางหัวใจและหลอดเลือด แมกนีเซียมสามารถช่วยการทำงานของเซลล์เยื่อบุหลอดเลือดแดงให้ดีขึ้น ปัจจุบันยังไม่มีหลักฐานชัดเจนสำหรับประโยชน์ของแมกนีเซียมในผู้ป่วยโรคไตเรื้อรังระยะท้าย การศึกษาวิจัยนี้แสดงผลของแมกนีเซียมต่อการทำงานของเซลล์เยื่อบุหลอดเลือดแดงในผู้ป่วยโรคไตเรื้อรังระยะ 4
วิธีการศึกษา: ผู้ป่วยโรคไตเรื้อรังระยะ 4 จำนวน 21 จะถูกสุ่มให้ได้รับการรักษามาตรฐานร่วมกับการเสริมแมกนีเซียม หรือ ได้รับการรักษามาตรฐานโดยไม่ได้รับการเสริมแมกนีเซียม และติดตามผู้ป่วยนาน 6 เดือน ผลการศึกษาหลักคือการเปลี่ยนแปลงของค่า flow mediated dilatation (FMD) และผลการศึกษารองคือการเปลี่ยนแปลงความดันโลหิต และการเกิดอาการไม่พึงประสงค์
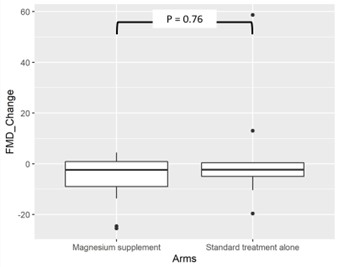
ผลการศึกษา: ผู้ป่วย 10 คนจาก 21 คนถูกสุ่มเข้ากลุ่มการรักษามาตรฐาน และ ผู้ป่วย 11 คน ถูกสุ่มเข้ากลุ่มการรักษามาตรฐานร่วมกับการเสริมแมกนีเซียม ค่าเฉลี่ยการเปลี่ยนแปลงของ FMD คือ -2.35 (IQR 10.6) ในกลุ่มการรักษามาตรฐานและ -2.4 (IQR 15.06) ในกลุ่มที่ได้รับการรักษามาตรฐานร่วมกับการเสริมแมกนีเซียม ซึ่งไม่มีความแตกต่างกันอย่างมีนัยทางสถิติ ค่าเฉลี่ยการเปลี่ยนแปลงความดันโลหิตซิสโตลิคลดลงทั้ง 2 กลุ่ม แต่ไม่มีความแตกต่างอย่างมีนัยสำคัญทางสถิติ (P=0.77) ค่าเฉลี่ยความดันไดแอสโตลิคเพิ่มขึ้นในกลุ่มการรักษามาตรฐาน (2.6 มิลลิเมตรปรอท, ค่าเบี่ยงเบนมาตรฐาน ±2.2) และลดลงในกลุ่มที่ได้รับการรักษามาตรฐานร่วมกับการเสริมแมกนีเซียม (-13.45 มิลลิเมตรปรอท, ค่าเบี่ยงเบนมาตรฐาน ±3.8) ซึ่งมีความแตกต่างกันอย่างมีนัยสำคัญทางสถิติ (P=0.002) ไม่พบผู้ป่วยที่มีอาการไม่พึงประสงค์ทั้ง 2 กลุ่ม
สรุป: การศึกษาไม่พบประโยชน์ของแมกนีเซียมต่อการทำงานของเซลล์เยื่อบุหลอดเลือดแดงด้วยการวัด FMD และความดันโลหิตซิสโตลิค แต่มีผลลดความดันไดแอสโตลิค
Article Details

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
บทความนี้ตีพิมพ์ภายไต้การอนุญาต CC BY-NC-ND 4.0 ซึ่งอนุญาตให้สามารถใช้บทความนี้พื่อวัตถุประสงค์ใดๆ ก็ตามที่ไม่ใช่เชิงพาณิชย์ โดยต้องมีการอ้างถึงที่มาของบทความอย่างครบถ้วน ใครก็ตามสามารถคัดลอกและแจกจ่ายทุกส่วนของบทความนี้โดยไม่ต้องขออนุญาตจากผู้ประพันธ์หรือสมาคมโรคไตแห่งประเทศไทย
เอกสารอ้างอิง
Michiels C. Endothelial cell functions. J Cell Physiol.2003; 196(3):430–43.
Lerman Amir, Zeiher Andreas M. Endothelial Function. Circulation. 2005;111(3):363–8.
Grover-Páez F, Zavalza-Gómez AB. Endothelial dysfunction and cardiovascular risk factors. Diabetes Res Clin Pract. 2009;84(1):1–10.
Favarato D, da Luz PL. Chapter 34 - Endothelial Function and Cardiovascular Risk Factors. In: Da Luz PL, Libby P, Chagas ACP, Laurindo FRM, editors. Endothelium and Cardiovascular Diseases [Internet]. Academic Press; 2018 [cited 2021 Apr 18]. p. 513–26. Available from: https://www.sciencedirect.com/science/article/pii/B9780128123485000349
Wu-Wong JR. Endothelial dysfunction and chronic kidney disease: treatment options. Curr Opin Investig Drugs Lond Engl 2000. 2008;9(9):970–82.
Annuk M, Soveri I, Zilmer M, Lind L, Hulthe J, Fellström B. Endothelial function, CRP and oxidative stress in chronic kidney disease. J Nephrol. 2005;18(6):721–6.
Zoccali C. Endothelial Dysfunction and the Kidney: Emerging Risk Factors for Renal Insufficiency and Cardiovascular Outcomes in Essential Hypertension. J Am Soc Nephrol. 2006;17(4 suppl 2):S61–3.
Recio-Mayoral A, Banerjee D, Streather C, Kaski JC. Endothelial dysfunction, inflammation and atherosclerosis in chronic kidney disease--a cross-sectional study of predialysis, dialysis and kidney-transplantation patients. Atherosclerosis. 2011;216(2):446–51.
Su JB. Vascular endothelial dysfunction and pharmacological treatment. World J Cardiol. 2015;7(11):719–41.
ter Braake Anique D., Shanahan Catherine M., de Baaij Jeroen H.F. Magnesium Counteracts Vascular Calcification. Arterioscler Thromb Vasc Biol. 2017;37(8):1431–45.
Wolf FI, Trapani V, Simonacci M, Ferré S, Maier JA. Magnesium deficiency and endothelial dysfunction: is oxidative stress involved? Magnes Res. 2008;21(1):58–64.
Kostov K, Halacheva L. Role of Magnesium Deficiency in Promoting Atherosclerosis, Endothelial Dysfunction, and Arterial Stiffening as Risk Factors for Hypertension. Int J Mol Sci. 2018;19(6):1724.
Pearson PJ, Evora PR, Seccombe JF, Schaff HV. Hypomagnesemia inhibits nitric oxide release from coronary endothelium: protective role of magnesium infusion after cardiac operations. Ann Thorac Surg. 1998;65(4):967–72.
Massy ZA, Drüeke TB. Magnesium and outcomes in patients with chronic kidney disease: focus on vascular calcification, atherosclerosis and survival. Clin Kidney J.2012;5(Suppl_1):i52–61.
Flammer Andreas J., Anderson Todd, Celermajer David S., Creager Mark A., Deanfield John, Ganz Peter, et al. The Assessment of Endothelial Function. Circulation. 2012;126(6):753–67.
Tanaka Atsushi, Tomiyama Hirofumi, Maruhashi Tatsuya, Matsuzawa Yasushi, Miyoshi Toru, Kabutoya Tomoyuki, et al. Physiological Diagnostic Criteria for Vascular Failure. Hypertension. 2018;72(5):1060–71.
Cunha AR, D’El-Rei J, Medeiros F, Umbelino B, Oigman W, Touyz RM, et al. Oral magnesium supplementation improves endothelial function and attenuates subclinical atherosclerosis in thiazide-treated hypertensive women. J Hypertens. 2017;35(1):89–97.
Sakaguchi Y, Hamano T, Obi Y, Monden C, Oka T, Yamaguchi S, et al. A Randomized Trial of Magnesium Oxide and Oral Carbon Adsorbent for Coronary Artery Calcification in Predialysis CKD. J Am Soc Nephrol JASN. 2019;30(6):1073–85.
Stout M. Flow-mediated dilatation: a review of techniques and applications. Echocardiogr Mt Kisco N. 2009;26(7):832–41.
Thijssen DHJ, Black MA, Pyke KE, Padilla J, Atkinson G, Harris RA, et al. Assessment of flow-mediated dilation in humans: a methodological and physiological guideline. Am J Physiol - Heart Circ Physiol. 2011;300(1):H2–12.
Thai HT Guideline 2019.pdf [Internet]. [cited 2021 Apr 18]. Available from: http://www.thaiheart.org/images/column_1563846428/Thai%20HT%20Guideline%202019.pdf
CKD Evaluation and Management – KDIGO [Internet]. [cited 2021 Apr 18]. Available from: https://kdigo.org/guidelines/ckd-evaluation-and-management/
