
Clinical Outcomes of Methanol Intoxication Outbreak Managed with Hemodialysis at Nopparat Rajathanee Hospital: Case Series and Literature Review
Article Sidebar
Main Article Content
Abstract
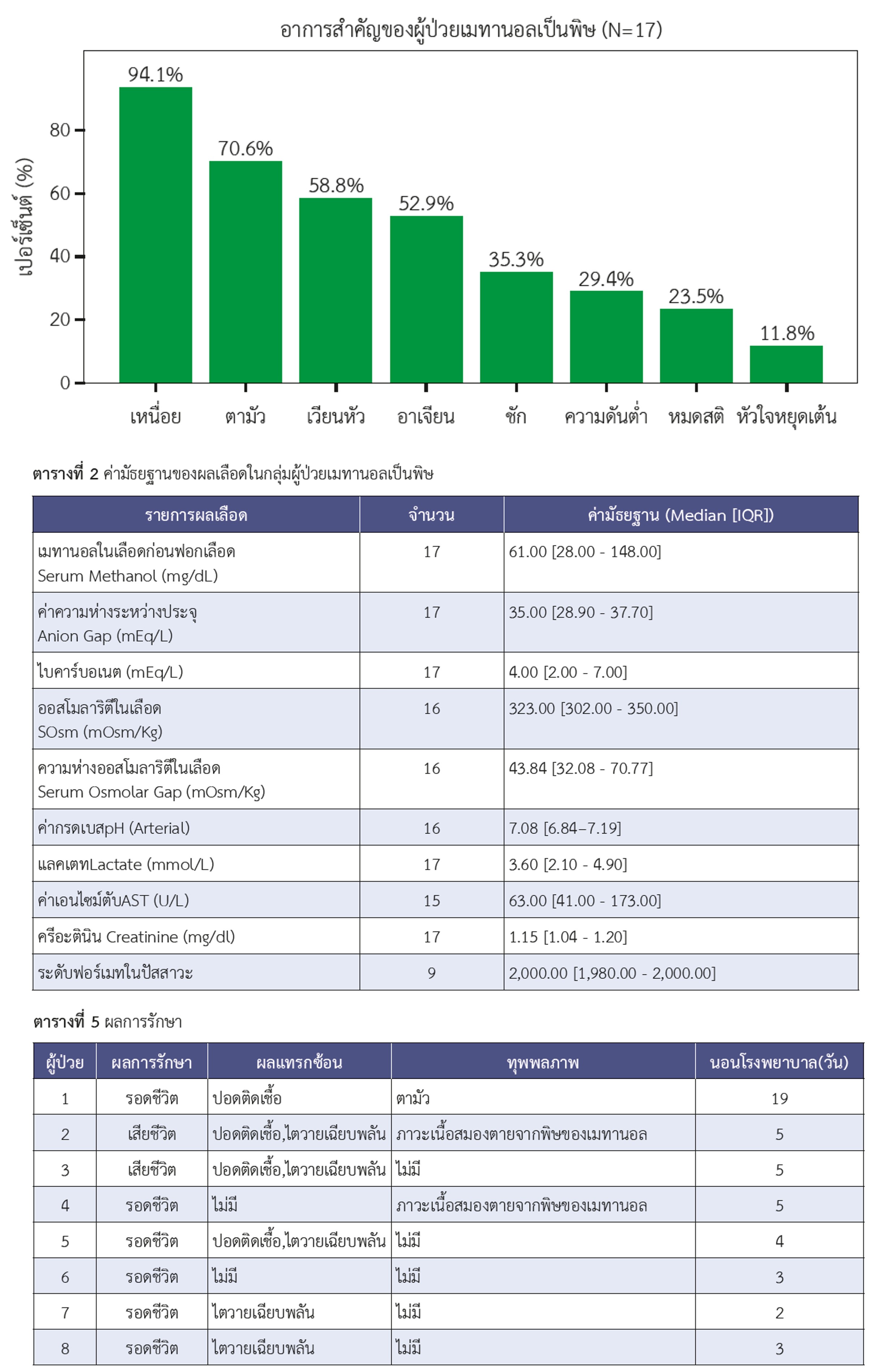
Following a mass methanol poisoning outbreak from illicit liquor in Bangkok in August 2024, hemodialysis became the primary life-saving treatment due to the unavailability of fomepizole in Thailand. This case series describes the baseline characteristics, biochemical parameters, treatment modalities, and clinical outcomes of patients with methanol poisoning treated with hemodialysis at a quaternary care hospital under the Ministry of Public Health in Bangkok, Thailand. Between August 22 and September 3, 2024, a total of 17 confirmed cases of methanol intoxication were identified. Most patients (94.1%) were male. The most common presenting symptoms were dyspnea (94.1%) and blurred vision (70.6%). Laboratory findings demonstrated severe metabolic acidosis, with a median pH of 7.08, serum bicarbonate of 4.0 mEq/L, and an anion gap of 35.0 mEq/L. All patients (100%) underwent intermittent hemodialysis, while 35.3% required additional continuous renal replacement therapy. The median door-to-dialysis time was 6 hours. The survival rate was 76.5% (13 cases), and the mortality rate was 23.5% (4 cases). Permanent disability occurred in 29.4% (5 cases), including permanent visual impairment (17.6%) and neurological deficits (11.7%). Early initiation of hemodialysis, combined with effective resource management during a mass casualty event, was a critical factor in achieving clinical outcomes comparable to international benchmarks
despite limited access to antidotes.
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This article is published under CC BY-NC-ND 4.0 license, which allows for non-commercial reuse of the published paper as long as the published paper is fully attributed. Anyone can share (copy and redistribute) the material in any medium or format without having to ask permission from the author or the Nephrology Society of Thailand.
References
Paasma R, Hovda KE, Jacobsen D. Methanol poisoning and long term sequelae – a six years follow-up after a large methanol outbreak. BMC Clin Pharmacol. 2009;9:5. doi: 10.1186/1472-6904-9-5.
Dejburum P, Sansinlapin C, Chantian T. A study of methanol poisoning outbreak from infused liquor in three communities, Chonburi, Thailand. Mahasarakham Hosp J. 2024;21(3):151-63.
Onyekwelu KC. Ethanol. In: Taukeni SG, editor. Psychology of Health - Biopsychosocial Approach. London: IntechOpen;2019. doi:10.5772/intechopen.79861.
Nekoukar Z, Zakariaei Z, Taghizadeh F, Musavi F, Banimostafavi ES, Sharifpour A, et al. Methanol poisoning as a new world challenge: A review. Ann Med Surg (Lond). 2021;66:102445. doi:10.1016/j.amsu.2021.102445.
EMACC-Emergency Medicine Anaesthesia Critical Care Working Group. Methanol Poisoning. [Internal Document/Guideline]. 2023.
Jangjou A, Moqadas M, Mohsenian L, Kamyab H, Chelliapan S, Alshehery S, et al. Awareness raising and dealing with methanol poisoning based on effective strategies. Environ Res. 2023;228:115886. doi:10.1016/j.envres.2023.115886.
Kraut JA. Approach to the treatment of methanol intoxication. Am J Kidney Dis. 2016;68(1):161-7. doi:10.1053/j.ajkd.2016.02.058.
Mullins ME, Kraut JA. The Role of the Nephrologist in Management of Poisoning and Intoxication: Core Curriculum 2022. Am J Kidney Dis. 2022;79(6):877-89. doi:10.1053/j.ajkd.2021.06.030.
Brent J, McMartin K, Phillips S, Aaron C, Kulig K. Fomepizole for the treatment of methanol poisoning. N Engl J Med. 2001;344(6):424-9. doi:10.1056/NEJM200102083440605.
Chan APL, Chan TYK. Methanol as an unlisted ingredient in supposedly alcohol-based hand rub can pose serious health risk. Int J Environ Res Public Health. 2018;15(7):1440. doi:10.3390/ijerph15071440.
Ashurst JV, Schaffer DH, Nappe TM. Methanol toxicity [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [cited 2026 Jan 28]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482121/.
Gonda A, Gault H, Churchill D, Hollomby D. Hemodialysis for methanol intoxication. Am J Med. 1978;64(5):749-58. doi:10.1016/0002-9343(78)90513-2.
Kellett J. What is the ideal triage process and the resources it requires? Lancet Reg Health West Pac. 2021;13:100203. doi:10.1016/j.lanwpc.2021.100203.
Gilboy N, Tanabe P, Travers D, Rosenau A. Emergency Severity Index (ESI): A Triage Tool for Emergency Department Care, Implementation Handbook 2020 Edition. Rockville (MD): Agency for Healthcare Research and Quality; 2020.
Roberts DM, Yates C, Megarbane B, Winchester JF, Maclaren R, Gosselin S, et al. Recommendations for the role of extracorporeal treatments in the management of acute methanol poisoning: a systematic review and consensus statement. Crit Care Med. 2015;43(2):461-72. doi:10.1097/CCM.0000000000000708.
Barceloux DG, Bond GR, Krenzelok EP, Cooper H, Vale JA. American Academy of Clinical Toxicology practice guidelines on the treatment of methanol poisoning. J Toxicol Clin Toxicol. 2002;40(4):415-46. doi:10.1081/CLT-120006745.
Lachance P, Mac-Way F, Desmeules S, De Serres SA, Julien AS, Douville P, et al. Prediction and validation of hemodialysis duration in acute methanol poisoning. Kidney Int. 2015;88(5):1170-7. doi:10.1038/ki.2015.232.
Zakharov S, Pelclova D, Navratil T, Belacek J, Kurcova I, Komzak O, et al. Intermittent hemodialysis is superior to continuous veno-venous hemodialysis/hemodiafiltration to eliminate methanol and formate during treatment for methanol poisoning. Kidney Int. 2014;86(1):199-207. doi:10.1038/ki.2014.60.
Zakharov S, Pelclova D. Czech mass methanol outbreak 2012: Epidemiology, challenges and clinical features. Clin Toxicol (Phila). 2014;52(10):1013-24. doi:10.3109/15563650.2014.974106.
Muchemi OM, Wanyonyi AW, Ogendo AF, Kasera K, Wilson G, Boru W, et al. Methanol Poisoning in Various Counties of Kenya, 2014. Int J Sci Res Publ. 2017;7(5):432-448.
