
Vitamin A Deficiency-induced Keratomalacia Due to Malabsorption Syndrome
Article Sidebar
Main Article Content
Abstract
Background: Keratomalacia is commonly reported in regions with high levels of malnutrition. We present a rare case of Vitamin A deficiency-induced keratomalacia due to malabsorption syndrome in Brunei Darussalam, a country with one of the highest per-capita gross domestic products in Southeast Asia - highlighting the importance of considering nutritional deficiencies even in affluent settings.
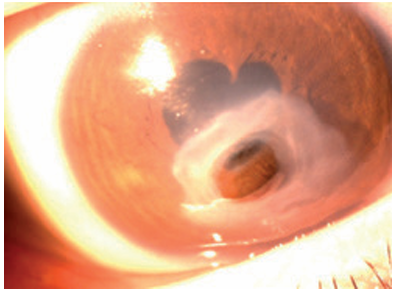
Case presentation: An 18-year-old Malay male presented with right eye redness, congestion and hand movement vision. He had atopic dermatitis, asthma, hyper Ig E syndrome, and multiple vitamin deficiencies, including vitamin D, vitamin B12, and iron. He was HLA dQ8 and DQ7 positive, DQ7 being a risk allele for coeliac disease. On initial examination, there was a right shield ulcer, which was treated for vernal atopic keratoconjunctivitis. Over a period of one month his skin and eye condition worsened, with xerosis of the conjunctiva, corneal thinning, perforation of corneal shield ulcer with an iris plug and shallowed anterior chamber. The clinical signs strongly suggest Vitamin A deficiency causing keratomalacia. He was admitted for systemic steroid treatment and given conservative intensive treatment of lubricants and topical antibiotics (moxifloxacin, tobramycin, and atropine). At six months review, and through a comprehensive treatment approach including Vitamin A supplements, carotenoid-rich food, the patient demonstrated a remarkable restoration of visual acuity of 6/9 in the affected eye.
Conclusion: Although Vitamin A deficiency is more common in developing countries, this case highlights that it can occur in a socioeconomically developed setting and may present with atypical features. Thorough history taking and clinical correlations are important to guide timely diagnosis and management in similar cases. Early recognition and prompt intervention are crucial to prevent irreversible visual loss.
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
References
Song P, Adeloye D, Li S, et al. The prevalence of vitamin A deficiency and its public health significance in children in low- and middle income countries: A systematic review and modelling analysis. J Glob Health. 2023;13:04084.
Chae T. Vitamin A deficiency in patients with a remote history of intestinal surgery. Br J Ophthalmol. 2006;90(8):955-956.
Sommer A. Vitamin A deficiency and its consequences. WHO. 1995;3.
Sommer A. Effects of Vitamin A Deficiency on the Ocular Surface. Ophthalmol. 1983;90(6).
Livingstone C, Davis J, Marvin V, Morton K. Vitamin A deficiency presenting as night blindness during pregnancy. Ann Clin Biochem. 2003;40(3).
Singh A, Maurya OPS, Jagannadhan MV, Patel A. Matrix metalloproteinases (MMP-2 and MMP-9) activity in corneal ulcer and ocular surface disorders determined by gelatin zymography. J Ocul Biol Dis Infor. 2012;5(2).
Sommer A, Green WR, Kenyon KR. Bitot’s Spots Responsive and Nonresponsive to Vitamin A: Clinicopathologic Correlations. Arch Ophthalmol. 1981;99(11).
WHO. Guideline: updates on the management of severe acute malnutrition in infants and children, Geneva: World Health Organization; 2013. Guideline: updates on the management of severe acute malnutrition in infants and children, Geneva: World Health Organization; 2013. 2013;(August 2013).
